-
Posted on January 19th, 2016
Brian
The following drawing shows the basic mechanics relating to shaking a baby. Surprisingly, the total shaking movement of the child’s body, to and fro, is only about 6″ (150mm). Just try it and see, (but not on a real child, please) and you will find it difficult and uncomfortable to make it more than that. You should also realise that it’s the child’s body that is shaken, not it’s head.
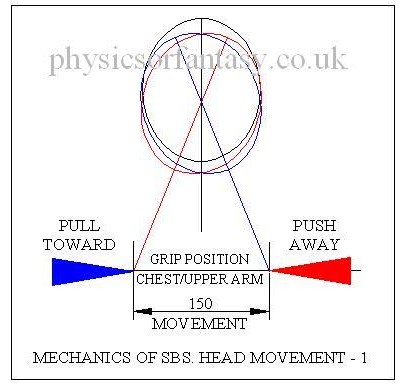
As the head is not rigidly fixed to the body it does not move this same 6″ but moves up and down by a few millimetres and also rotates by about 20º each side of the vertical, the neck bending to allow this to happen. There are only small acceleration forces acting on the head. Basically, the body moves relative to an almost stationary head
The inertia of the child’s head restricts any rapid movements to it. Any movements of the head can only be caused by forces acting through the neck, which is very flexible. Any serious movements to the head would cause serious damage to the spine which is just as fragile as the brain.
The following drawing refers to the auxiliary head movements that should also be considered.
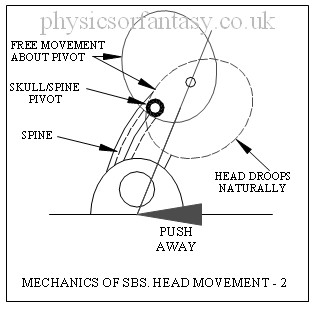
The relatively free ‘nodding’ movement of the head is entirely consciously controlled by muscles in the neck. If you fall asleep your head will freely fall backwards, sideways or forward. Undue accelerations in this movement would likely cause neck muscle and tendon damage plus damage to the complex pivot assembly because in the SBS case the child is assumed to be awake. However, these same injuries could also happen during the birth process.
I sent data to the Louise Woodward defence team relating to the mechanics of Shaken Baby Syndrome in 1997.
Anyone who watched the case on television, after the defence team brought in a specialist engineer, must have been amazed by the prosecution attorney’s ridiculous antics whilst attempting to show how the head could be held in such a way that it was shaken along with the body. She had obviously spent a lot of time thinking about this, but the contortions she got into made it obvious that Louise Woodward could never have carried out the same rigmarole in a fit of anger.
———————————–
Abstract.
Dynamic Biomechanical Findings on Shaken Baby Syndrome/Lethal Minor Falls
http://sbsreferences.com/DownloadHandler.ashx?pg=392f9051-f6fa-4a54-a2d8-70157cf253c0§ion=11dab90f-171c-4263-9334-b175c406f533&file=Exhibit+14A.pdf
FROM: Injury Biomechanics Researcher: Chris Van Ee, PhD
TO: The Honorable Court
SUBJECT: Dynamic Biomechanical Findings on SBS-LMF
DATE: March 3, 2008
Dynamic Biomechanical Findings March 7, 2008 Page 2 of 4
2. SBS/LMF Findings From Biomechanical Tests and Studies:
(A) Scientific testing has shown that head acceleration levels from anterior/posterior human shaking of a normal 0- to 2-year-old child in the sagittal plane results in head acceleration and force levels that are much lower than those which are associated with traumatic head injury. Repeated testing of this hypothetical has shown that the head accelerations associated with shaking are far below the level associated with injury and there is no quality data to support the SBS brain injury mechanism. Thus shaking, even if done in a fit of anger, is not expected to result in head dynamics sufficient to cause direct intracerebral trauma.
(B) Human shaking (id.) may cause lethal brain stem and cervical spine injuries in a 0-to 2-year-old child, as the forces necessary for these injuries are well below the level needed for fatal brain injuries and are consistent with the forces that can be produced in shaking. Put another way, these neck injuries would be expected in any hypothetical-superhuman-strength case of SBS where superhuman dynamics resulted in head accelerations leading to intercerebral trauma (if SBS were valid, which it is not).
————————————–
Abstract from
Shaken baby syndrome: A biomechanics analysis of injury mechanisms.
Traumatic infant shaking has been associated with the shaken baby syndrome (SBS) diagnosis without verification of the operative mechanisms of injury. Intensities for SBS have been expressed only in qualitative, unsubstantiated terms usually referring to acceleration/deceleration rotational injury and relating to falls from great heights onto hard surfaces or from severe motor vehicle crashes. We conducted an injury biomechanics analysis of the reported SBS levels of rotational velocity and acceleration of the head for their injury effects on the infant head-neck. Resulting forces were compared with experimental data on the structural failure limits of the cervical spine in several animal models as well as human neonate cadaver models. We have determined that an infant head subjected to the levels of rotational velocity and acceleration called for in the SBS literature, would experience forces on the infant neck far exceeding the limits for structural failure of the cervical spine. Furthermore, shaking cervical spine injury can occur at much lower levels of head velocity and acceleration than those reported for the SBS. These findings are consistent with the physical laws of injury biomechanics as well as our collective understanding of the fragile infant cervical spine from (1) clinical obstetric experience, (2) automotive medicine and crash safety experience, and (3) common parental experience. The findings are not, however, consistent with the current clinical SBS experience and are in stark contradiction with the reported rarity of cervical spine injury in children diagnosed with SBS. In light of the implications of these findings on child protection and their social and medico-legal significance, a re-evaluation of the current diagnostic criteria for the SBS and its application is suggested.
Faris A. Bandak. Department of Neurology, A1036 F. Edward Hébert School of Medicine, Uniformed Services, University of the Health Sciences, Bethesda, MD 20814, USA
—————————-
Abstract from Wikapedia/cheshire nanny case (Louise Woodward Trial. 1967)
Patrick Barnes, a pediatric radiologist at Stanford University, was a key prosecution witness in the trial, but in 2011 said he would not give the same testimony today. He said there had been a revolution in the understanding of head injuries in the past decade, partly due to advances in MRI brain scanning technology: “We started realizing there were a number of medical conditions that can affect a baby’s brain and look like the findings that we used to attribute to shaken baby syndrome or child abuse”, such as infections and in utero strokes.
—————————-
MORE TO FOLLOW SHORTLY.
Author – Brian Williams
Read also; Shaken Baby Syndrome-Debunking the Myth
Shaken baby syndrome: A biomechanics analysis of injury mechanisms
-
Posted on January 2nd, 2016
Brian
Birth Brain Injuries
1. What is a ‘normal’ birth?
Figures given in ‘ESSENTIAL OBSTETRICS & GYNAECOLOGY’ (E.O.G.) Chapter 17, indicate that 6.7% of live births in England & Wales are Low Birth Weight i.e. less than 2.5 kilograms.
From the same chapter we are told that the common causes of death in the 1st 4 weeks of life are;
1. Major congenital abnormalities incompatible with life.
2. Prematurity- the most important single factor in causing neonatal death, associated with,
a. Respiratory Distress Syndrome.
b. Pnuemonia.
c. Intercranial Haemorrhage and cerebral damage sustained either during labour and delivery or in the early neonatal period.
d. Necrotizing enterocolitus.
From NEONATAL NEUROLOGY page 139, we are told that ” Levene and Starte (1981) studied 202 consecutive admissions of all birth weights, 68 (34%) of whom were found to have intracranial haemorrhage”
From NEONATAL NEUROLOGY page 76, we are told that approx. 27% of premature infants born in the 31st to 34th weeks develop Periventricular haemorrhages.
From NEONATAL NEUROLOGY ,page 63, we are told that approx. 7% of premature infants born with a birth weight of 1.8 kilograms or less have subarachnoid haemorrhage.
From NEONATAL NEUROLOGY page 57, we are told that ” Intracranial haemorrhage occurs commonly in newborn infants and is an important cause of death & handicap.”
It is evident therefore, that brain haemorrhages in infants is common.
It is also a well documented fact that due to the lack of development of the blood vessels the premature infant is at an increased risk of haemorrhage.
Subdural Haematomas.
From NEONATAL NEUROLOGY, page 58, we are told that “the cause of this type of condition is usually traumatic, that the incidence of it has greatly reduced over recent years and that It has not however, completely disappeared; indeed it may still be a relatively common lesion affecting the neonatal brain and may be associated with few clinical signs, thus remaining undiagnosed during life.”
I need to tidy up the following two graphics and information on originators. Brian.
Intracranial Haemorrhages
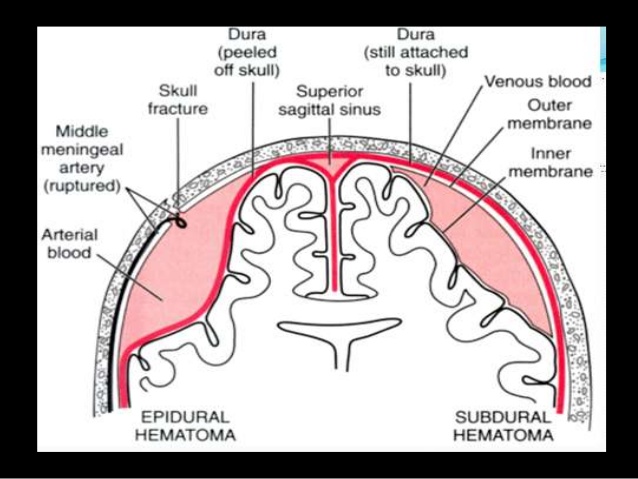
Note the difference between the following two sets of statements referring to the cause of subdural haemorrhages.
 The first is a bit confusing (like most medical literature) but I read this as 1. Actual damage to the head. 2. Caused by distortion of the brain during the birth process.
The first is a bit confusing (like most medical literature) but I read this as 1. Actual damage to the head. 2. Caused by distortion of the brain during the birth process.
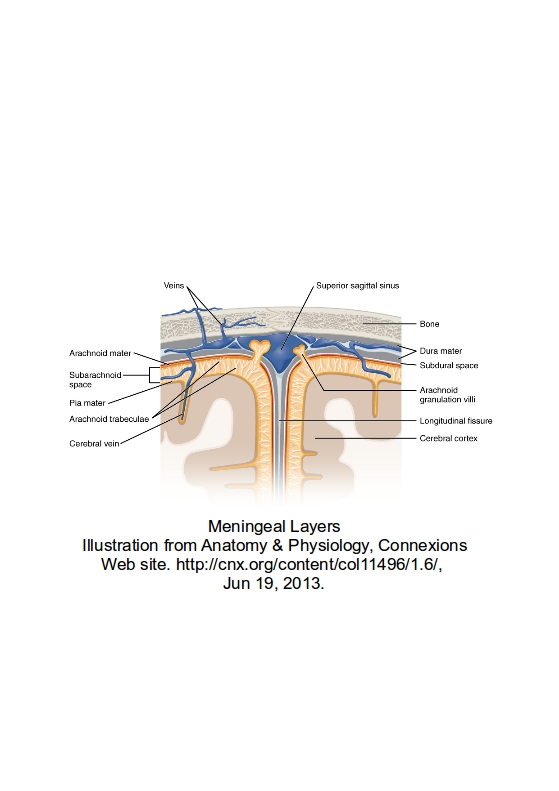
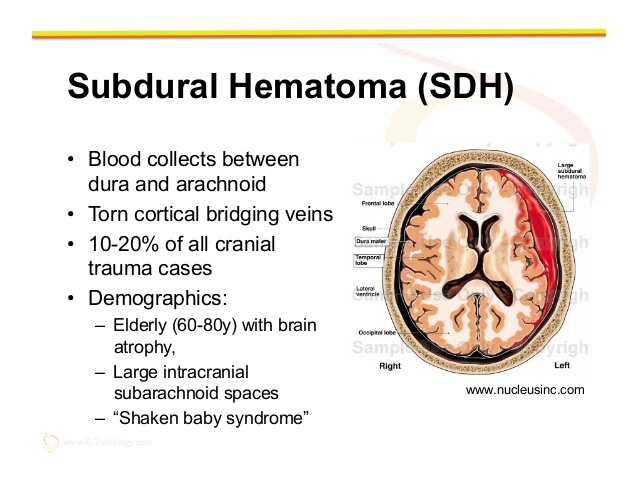
The second set of statements is also slightly confusing, but I read this as “Blood collects between the dura and arachnoid layers, due to torn veins. Subdural Haematomas comprise 10 – 20% of all cranial trauma cases.
The three main causes of the torn veins is 1. Brain atrophy in the elderly. 2. Large intracranial subarachnoid spaces.
3. “Shaken Baby Syndrome”.
Relating to demographics, it should read. 1. Elderly people with brain atrophy. 2. People with large intracranial subarachnoid spaces. 3. “Shaken Baby Syndrome” is not a demographic type.
There can be many causes of subdural haemotomas to people who are not between the ages of 60-80 with brain atrophy, or people who have large intracranial subarachnoid spaces.
Falls can occur to people of all ages. Are the paediatricians really asking us to believe, that subdural Haematomas only happen to the people mentioned in the above two demographic categories plus babies that are shaken or thrown about? If a 30year old man falls off a ladder, are the paediatricians saying that the man cannot suffer from a subdural Haematomas due to falling?
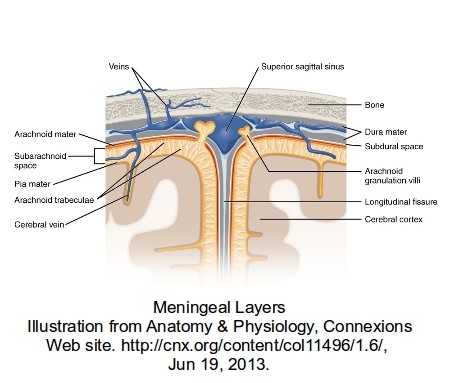
In the drawing below there are numerous large and small veins shown. During the birth process the head can get quite seriously distorted, because at this stage the skull is quite soft and pliable to enable the head to pass through the birth canal.
 Excluding any accelerations or decelerations (obviously not applicable during the birth process unless the paediatrician is (non-accidentally) shaking the mother or throwing her onto the floor), the main stresses are distortions to the head caused primarily by the natural pressure of the birth process working against the restriction of the birth canal. It should be remembered that the skull is not bone at this stage, and although giving some protection to the brain, is not a crash helmet. In the area of the fontanelle, the very soft area of the skull in babies, the brain is virtually unprotected.
Excluding any accelerations or decelerations (obviously not applicable during the birth process unless the paediatrician is (non-accidentally) shaking the mother or throwing her onto the floor), the main stresses are distortions to the head caused primarily by the natural pressure of the birth process working against the restriction of the birth canal. It should be remembered that the skull is not bone at this stage, and although giving some protection to the brain, is not a crash helmet. In the area of the fontanelle, the very soft area of the skull in babies, the brain is virtually unprotected.
Squeezing of the brain tends to to force it forward and bulge into the fontanelle area, but being restrained by the dura-mater. This will cause stretching on the inside of the dura-mater that can damage veins and capillaries that then bleed into the subdural space.
Obviously there are many things to consider; Is it a rapid/easy birth or an extended/complicated birth? Is it a full term baby or premature? How much external handling of the birth was required?
The birth process is not a guaranteed simple process especially in a first birth for the mother. The mother’s natural anxiety with her first birth can complicate the process. The mother’s anatomy can have a great effect on the birth process.
Jaundice Causes
By Mayo Clinic Staff
Excess bilirubin (hyperbilirubinemia) is the main cause of jaundice. Bilirubin, which is responsible for the yellow color of jaundice, is a normal part of the pigment released from the breakdown of “used” red blood cells.
Normally, the liver filters bilirubin from the bloodstream and releases it into the intestinal tract. A newborn’s immature liver often can’t remove bilirubin quickly enough, causing an excess of bilirubin. Jaundice due to these normal newborn conditions is called physiologic jaundice, and it typically appears on the second or third day of life.
Other causes
An underlying disorder may cause jaundice. In these cases, jaundice often appears much earlier or much later than physiologic jaundice. Diseases or conditions that can cause jaundice include:
-
Internal bleeding (hemorrhage)
-
An infection in your baby’s blood (sepsis)
-
Other viral or bacterial infections
-
An incompatibility between the mother’s blood and the baby’s blood
-
A liver malfunction
-
An enzyme deficiency
-
An abnormality of your baby’s red blood cells that causes them to break
—————————————
From. wikipedia.org/wiki/Shaken_baby_syndrome/legal issues
In 2012, Dr. A. Norman Guthkelch, the neurosurgeon often credited with “discovering” the diagnosis of SBS,[54] published an article “after 40 years of consideration,” which is harshly critical of shaken baby prosecutions based solely on the triad of injuries.[55] Again, in 2012, Dr. Guthkelch stated in an interview, “I think we need to go back to the drawing board and make a more thorough assessment of these fatal cases, and I am going to bet . . . that we are going to find in every – or at least the large majority of cases, the child had another severe illness of some sort which was missed until too late.”[56] Furthermore, in 2015, Dr. Guthkelch went so far as to say, “I was against defining this thing as a syndrome in the first instance. To go on and say every time you see it, it’s a crime…It became an easy way to go into jail.”[57]
On the other hand, Teri Covington, who runs the National Center for Child Death Review Policy and Practice, worries that such caution has led to a growing number of cases of child abuse in which the abuser is not punished.[54]
This is a rather nasty statement (by Teri Covington) to make. She is implying that irrespective of the evidence, the people charged with SBS are actually the abusers. Brian.
———————————–
More to follow
——————————————
Author; Brian Williams.
-
Posted on December 22nd, 2015
Brian
The original “Shaken Baby Syndrome” was a logical and sensible set of guide lines. These were changed over the years to include injuries that previously were known and accepted as birth injuries. Over the last 20 years these later, suspect, injuries have virtually replaced the original guide lines, and in the majority of ‘ Shaken Baby’ cases there is no evidence that indicates that shacking has taken place. I originally became involved in this problem in 1996 and supplied some data to the “Cheshire Nanny, Louise Woodward” defence team. (I watched a considerable amount of the court proceedings and in my opinion the court case was a legal and medical fiasco.)
Note that the accelerations claimed by paediatricians to cause bleeding in the brain, cannot be obtained by shaking without damage to the neck. Basic mechanics, not a subject understood by them.
Brian.
SEE MORE ON THIS SUBJECT ON THIS WEBSITE:
The Mechanics of the Shaken Baby Syndrome
Birth Brain Injuries
External injuries and disappearing bruises
Strange statements made by medical experts
Expert Witnesses.
Shaken Baby Syndrome and the Justice System.
Retinal Haemorrhages.
Shaken Baby Syndrome facts and fallacies.
————————————————
From the Daily Telegraph 22nd December 2015
Dr Waney Squier, a paediatric neuropathologist, is due to appear before the General Medical Council (GMC) tomorrow accused of “bias” and “dishonesty” after disputing the existence of “shaken baby syndrome” in a number of court cases.
For decades, the pathologist, who works at the John Radcliffe Hospital, Oxford, appeared as a prosecution witness against parents accused of killing their children.
She argued that a combination of three brain injuries — swelling of the brain, bleeding between the skull and brain and bleeding in the retina — was sufficient to determine that the death resulted from a child being violently shaken.
But more than a decade ago, amid the emergence of research disputing the mainstream theory, Dr Squier had a change of heart, becoming convinced that such symptoms were not conclusive.
Fearing that reliance on the argument had led to miscarriages of justice, she became a key expert witness defending parents who said their children’s deaths were the result of natural tragedies.
The case opening tomorrow could see Dr Squier, a pathologist for more than 30 years, removed from the medical register, for the opinions she has expressed in court.
The charges against her — of which few details have been released — have shocked several medical and legal specialists, who believe the action stems from a campaign to silence doubts about the theory, and secure more convictions for child murder.
Dr Marta Cohen, a paediatric pathologist at Sheffield Children’s Hospital who shares Dr Squier’s views, said: “I believe this humble, clever, courageous woman is the victim of a witch hunt by the Metropolitan Police to stop her from being an expert witness which may risk them losing their case.”
Dr Squier, 66, has devoted almost all of her professional life to the study of infant brains, appearing in courts around the world in cases where babies had died after suffering brain injury. In the UK, around 250 cases involving claims of shaken baby syndrome go to court a year.
Until 2001, she agreed with the standard medical view that the combination of three key symptoms, known as the “triad”, should lead to a conviction. But subsequent research led her to doubt that these symptoms alone were sufficient verification of guilt.
She came to believe that shaken baby syndrome may not exist, and that the triad signs could occur naturally in a baby. Dr Squier suggests that bleeding into the membranes in the brain could be a mechanism in young babies, which is intended to protect the brain itself from haemorrhage as it is exposed to pressure during delivery.
The view, shared by a minority of pathologists, is at odds with mainstream theories developed in the 1970s.
In 2000, Lorraine Harris, of Derbyshire, was jailed for manslaughter, after Dr Squier concluded her four-month-old baby Patrick had been shaken to death. But in a 2005 appeal, the pathologist was called as an expert witness for the defence, saying she was now convinced the criteria she had used to define whether shaken baby syndrome had occurred were wrong. The conviction was quashed.
Around the world, the arguments became heated. The case of British nanny Louise Woodward — found guilty in 1997 of shaking eight-month-old Matthew Eappen to death in Boston, Massachusetts — was pivotal in bringing arguments over shaken baby syndrome into the public eye. She was jailed for 15 years but the conviction for second degree murder was later reduced to involuntary manslaughter.
Dr Squier became the target of criticism. This culminated in a 2009 case in which a High Court judge, Justice Eleanor King, accused her of speaking “contrary to the mainstream of current thinking”. As a result, in April 2010, police referred the doctor to the GMC. Around the same time, Scotland Yard police are alleged to have undermined the pathologist and other expert witnesses blamed for failure to convict in cases of shaken baby syndrome.
At a US conference in 2010, Det Insp Colin Welsh, then of the Met’s child abuse investigation command, was reported to have suggested police would investigate such experts and report them to their professional bodies “to see if we turn up anything”.
Since then, the pathologist has been rejected by a number of courts. In 2011, Dr Squier said: “If I am blocked from giving evidence in court, defendants already having to cope with the tragic death of a baby will not get the benefit of the new science. Equally, if the courts fail to accept that the mainstream view of 30 years ago can no longer be relied upon, there will be serious miscarriages of justice.”
The pathologist said many convictions for shaken baby syndrome relied on confessions. “Some police grind those accused down interviewing them for hours while their baby is dying in hospital,” she said. “Under such duress people can confess to anything.”
Tomorrow, a GMC fitness to practise panel will consider charges that between 2007 and 2010, the pathologist failed to be “objective and unbiased”, was “dishonest”, and “brought the reputation of the medical profession into disrepute” while acting as an expert witness in court cases.
Last week, the GMC had yet to pass on to the pathologist’s lawyer full details of her alleged dishonesty. Dr Squier said: “I refute the charges absolutely. I will be putting up a very robust defence but I am unable to discuss it further at the moment.”
If she is cleared, it could throw the findings of thousands of cases into question.
Prof Margaret Esiri, emeritus professor of neuropathology at the University of Oxford, who has worked with Dr Squier since the 1980s, said: “Her findings do make it more difficult for the police to prosecute. They would rather evidence was cut and dried so they can get their convictions.”
Bill Bache, a solicitor who has defended families in cases where shaken baby syndrome was alleged, said he was “flabbergasted” by the charges.
Clive Stafford Smith, a civil rights lawyer and director of the charity Reprieve, said: “Much shaken baby and battered child testimony is extremely dubious, and should be vigorously questioned.”
The Medical Practitioners Tribunal Service, which manages such GMC hearings, declined to comment. The Metropolitan Police said: “We are aware of a report registered by the then National Police Improvement Agency with the GMC in 2010 about a doctor. The Metropolitan Police cooperated with a request from the GMC to provide relevant information.”
See also-
The Mechanics of the Shaken Baby Syndrome
Birth Brain Injuries
External injuries and disappearing bruises
Strange statements made by medical experts
Expert Witnesses.
Shaken Baby Syndrome and the Justice System.
Retinal Haemorrhages.
Shaken Baby Syndrome facts and fallacies.
-
Posted on March 19th, 2015
Brian
“The bruise on the knee is caused by strong gripping.” – Senior Consultant paediatrician.
This refers to a single bruise about 8-10mm dia, on the side of the child’s knee. This bruise was referred to on numerous medical reports. All the medical experts apparently agreed that it was caused by strong gripping.
Note: This bruise was the only one found on the child, apart from severe bruising around the head caused by the birth process. (This head bruising was photographed by the parents shortly after birth).
Later this same consultant referred to this bruise as “bruising around the knee caused by gripping”.
How does ‘strong gripping’ produce a single small bruise?
Statement of parents referring to this bruise; “our dog, a Staffordshire bull terrier, jumped up on to the settee and her paw caught the babies leg.”
Interpretations of this statement in reports given by various medical “experts” on the prosecution team.
A. “the dog jumping up on him and kicked him”. Consultant paediatrician who brought the charges.
B. “the dog jumped up, … her legs were out-stretched and one of them was touching the baby’s knee”. Senior Consultant paediatrician.
C. ” In my opinion the bruise on the knee is unlikely to be caused by the dog resting her feet on the baby in the manner described.” As above.
D. “and it is hard to see how a medium sized dog could land on a child’s knee with sufficient force to cause a bruise”. As above.
E. “the bruise on the knee is caused by tight gripping around the knee”. As above.
The Senior Consultant paediatrician referred to above was from a Children’s Hospital and in affect took over the prosecution.
Dogs have none-retractable claws. We had hoped that this particular consultant would allow us to walk the Staffordshire bull terrier across her naked legs during the court case.
The bruise was too small to have been caused by tight gripping by either of the parents, who were both over 6 feet tall. The bruise was consistent with an impact from a dogs claw.
Although this particular bruise was a genuine bruise that would be recognised as such by most people, various other ‘bruises’ were referred to by the prosecution. These arrived in the months waiting for the court case.
Disappearing Bruises.
Marks that are not bruises.
Petechial ” bruising”.
A very loose definition covering many different situations. If you rest your arm on a ribbed mat for a few minutes, you will find red lines on your arm. According to SBS “experts” this is caused by someone viciously shaking you or throwing you down onto a hard floor. An exaggeration? Yes, but only slightly.
These marks rapidly disappear because no damage has been caused, therefore they are not bruises. This type of marking is caused by pressure, not impact. In fact these marks are not actually ‘petechia’, nor do they have a “petechial appearance” as claimed by most of the paediatric prosecution ‘experts’.
Vasomotor lability
Vasomotor. Causing or relating to the constriction or dilatation of blood vessels.
Lability. Open to change; readily changeable or unstable.
Extract from Consultant Community Paediatrician’s report.
During my assessment, when I lay ******* on the rubber ridged mat to assess his locomotor development, I did notice when I picked him up that he had some red lines on his back which were the impressions from the mat. These disappeared within 5 minutes of finishing the examination.
I felt that this demonstrated a certain amount of vasomotor lability at the skin, but these were clearly not bruises which are caused by trauma and a bleeding into the skin.
This examination was carried out approximately 8.5 months after the child’s birth.
———————————————–
Petechiae Causes.
By Mayo Clinic Staff
Tiny blood vessels (capillaries) link the smallest parts of your arteries to the smallest parts of your veins. Petechiae appear when capillaries bleed, leaking blood into the skin. A number of things — including prolonged straining, certain medical conditions, specific types of injuries and some medications — can cause this bleeding.
—————————————————-
The parents took the baby to the family doctor because of a persistent sickness over a few days.
After the examination the doctor noted that red marks were on the baby’s back caused by lying on a ribbed examination table. This was shortly before the ambulance arrived at the surgery to take the baby and parents to the hospital.
At the hospital the baby was examined by two paediatricians. After this the parents were charged with shaking him.
Later reports supplied to the parents ., noted “Dr.********, my colleague, also noted some petechial bruising on the left upper arm…….”.
Why would he say this? He examined the baby quite soon after “his colleague”, so why did he not say that he himself had found these bruises?
There were no petechial bruises on the babies arms at the family doctors surgery, the parents and the baby were with the ambulance staff from the surgery to the hospital. So who caused these “life threatening” injuries due to throwing the baby about?
No subsequent examination found any evidence of this bruising, no member of the family saw this bruising and no photographs were taken of it. Petechial bruising does not just disappear, because it depends on damage to sub-cutaneous blood capillaries.
There “bruises” were marks left by normally handling of the baby, and rapidly disappeared. (Note: The baby was 9 weeks premature at birth). Neither of these two doctors mentioned these arm “bruises” after this report, but they were frequently referred to in other doctors reports and considered to be evidence.
It is a well documented medical fact that due to the lack of development of the blood vessels, the premature infant is at an increased risk of haemorrhage.
External Injuries.
The above mentioned bruise on the baby’s leg was the only external injury found at any time after the baby left hospital after the birth.
However, at birth there was a “very badly bruised head”, as noted by the midwife.
Not a ‘bruised head’, or a ‘badly bruised head’ but a ‘very badly bruised head’.
There was also a depression on the front right hand side of the head.
Author – Brian Williams.
-
Posted on March 6th, 2015
Brian
A. “The bruise on the knee is caused by strong gripping.” – Senior Consultant paediatrician.
This refers to a single bruise about 8-10mm dia, on the side of the child’s knee. This bruise was referred to on numerous medical reports. All the medical experts apparently agreed that it was caused by strong gripping.
Note: This bruise was the only one found on the child, apart from severe bruising around the head caused by the birth process. (This head bruising was photographed by the parents shortly after birth).
Later this same consultant referred to this bruise as “bruising around the knee caused by gripping”.
How does ‘strong gripping’ produce a single small bruise?
Statement of parents referring to this bruise; “our dog, a Staffordshire bull terrier, jumped up on to the settee and her paw caught the babies leg.”
Interpretations of this statement in reports given by various medical “experts” on the prosecution team.
A. “the dog jumping up on him and kicked him”. Consultant paediatrician who brought the charges.
B. “the dog jumped up, … her legs were out-stretched and one of them was touching the baby’s knee”. Senior Consultant paediatrician.
C. ” In my opinion the bruise on the knee is unlikely to be caused by the dog resting her feet on the baby in the manner described.” As above.
D. “and it is hard to see how a medium sized dog could land on a child’s knee with sufficient force to cause a bruise”. As above.
E. “the bruise on the knee is caused by tight gripping around the knee”. As above.
The Senior Consultant paediatrician referred to above was from a Children’s Hospital and in affect took over the prosecution.
Dogs have none-retractable claws. We had hoped that this particular consultant would allow us to walk the Staffordshire bull terrier across her naked legs during the court case.
The bruise was too small to have been caused by tight gripping by either of the parents, who were both over 6 feet tall. The bruise was consistent with an impact from a dogs claw.
Although this particular bruise was a genuine bruise that would be recognised as such by most people, various other ‘bruises’ were referred to by the prosecution. These arrived in the months waiting for the court case.
Disappearing Bruises.
Marks that are not bruises.
Petechial ” bruising”.
A very loose definition covering many different situations. If you rest your arm on a ribbed mat for a few minutes, you will find red lines on your arm. According to SBS “experts” this is caused by someone viciously shaking you or throwing you down onto a hard floor. An exaggeration? Yes, but only slightly.
These marks rapidly disappear because no damage has been caused, therefore they are not bruises. This type of petechia is caused by pressure, not impact.
———————————————–
Petechiae Causes.
By Mayo Clinic Staff
Tiny blood vessels (capillaries) link the smallest parts of your arteries to the smallest parts of your veins. Petechiae appear when capillaries bleed, leaking blood into the skin. A number of things — including prolonged straining, certain medical conditions, specific types of injuries and some medications — can cause this bleeding.
—————————————————-
The parents took the baby to the family doctor because of a persistent sickness over a few days.
After the examination the doctor noted that red marks were on the baby’s back caused by lying on a ribbed examination table. This was shortly before the ambulance arrived at the surgery to take the baby and parents to the hospital.
At the hospital the baby was examined by two paediatricians. After this the parents were charged with shaking him.
Later reports supplied to the parents ., noted “Dr.********, my colleague, also noted some petechial bruising on the left upper arm…….”.
Why would he say this? He examined the baby quite soon after “his colleague”, so why did he not say that he himself had found these bruises?
There were no petechial bruises on the babies arms at the family doctors surgery, the parents and the baby were with the ambulance staff from the surgery to the hospital. So who caused these “life threatening” injuries due to throwing the baby about?
No subsequent examination found any evidence of this bruising, no member of the family saw this bruising and no photographs were taken of it. Petechial bruising does not just disappear, because it depends on damage to sub-cutaneous blood capillaries.
There “bruises” were marks left by normally handling of the baby, and rapidly disappeared. (Note: The baby was 9 weeks premature at birth). Neither of these two doctors mentioned these arm “bruises” after this report, but they were frequently referred to in other doctors reports and considered to be evidence.
It is a well documented medical fact that due to the lack of development of the blood vessels, the premature infant is at an increased risk of haemorrhage.
————————————–
B. “Measurements of the baby’s head circumference during its stay in the Special Care Baby Unit at *******, demonstrate that *****’s head circumference increased at a normal rate during the first few weeks of life, and that **** head size was in proportion to body weight. ” – Senior Consultant paediatrician.
Why do I consider this to be a strange statement to make?
Because the baby’s head circumference was increasing at a rate twice that of a normal birth baby, 4 days before it was released from hospital into the parent’s care. Also, the weight was falling seriously relative to the guide curves (centile charts).
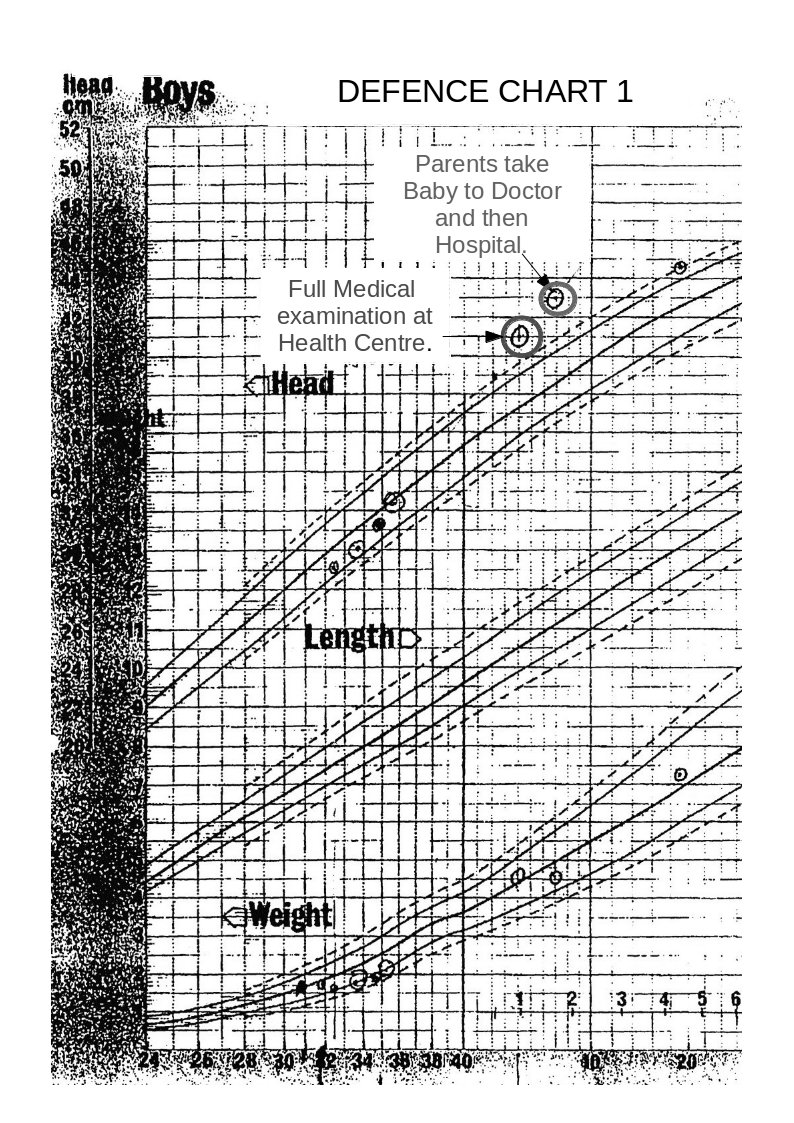
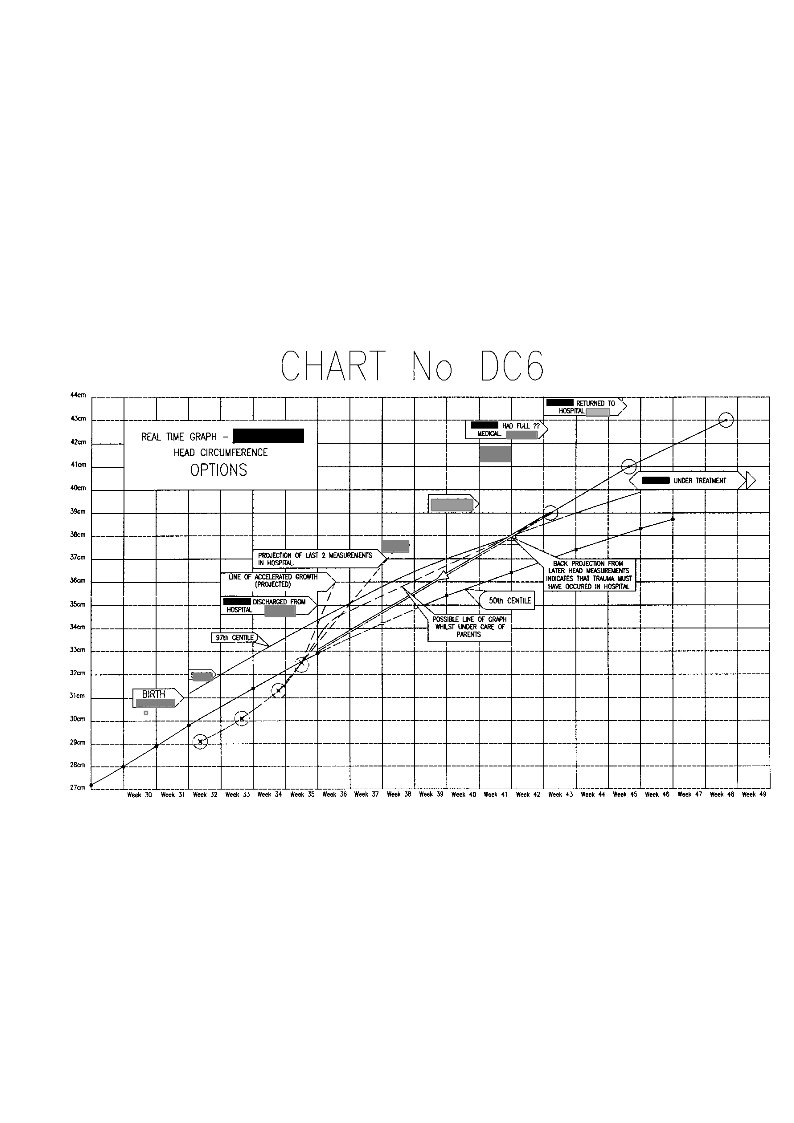
Defence Chart 1
Note; The above graph shows ‘Centile’ curves which are standard guide curves, used to monitor child growth. The centre line on each set of curves is the 50th centile (the ideal curve), the lower dashed line is the 10th centile and the solid line above this is the 25th centile. The upper dashed line is the 90th centile and the solid line below this is the 75th centile.
On the weight curves the measurements show that the child’s weight is actually falling relative to the 50th centile, and is in the danger area. (Whoever entered these point measurements obviously got them wrong at first and then corrected them.)
On the head measurement curves the figures indicate that the head diameter is rising.
In fact the head measurements between the last two made whilst the baby was still in hospital shows that the rise in the period was twice that of a normal ‘term’ baby.
Any doctor should have seen that this was a serious cause for concern.
Was this Senior Consultant Paediatrician lying?
Had this Senior Consultant Paediatrician not seen the charts?
I personally believe that the charts had not been seen.
Note on the above graph the two high-lighted measurements. The measurement taken at the heath centre, 3 weeks before the parents took the child to the doctor and hospital, shows that the head measurement was well above the 97th centile danger level at this time.
This timing is important and will be discussed later.
The defence team received a copy of this chart 5 months after the parents had been charged, despite constant requests for medical records.
The graph below shows a centile graph received at the same time as the previous chart, but obviously created at a later date. You will notice that there are differences.
The head circumferences figures are not now shown for the period from birth to leaving hospital. Also, the plotted point on Defence Chart 1 at the Medical Centre that was shown to be well above the danger level has now been moved down to the 90th centile line.
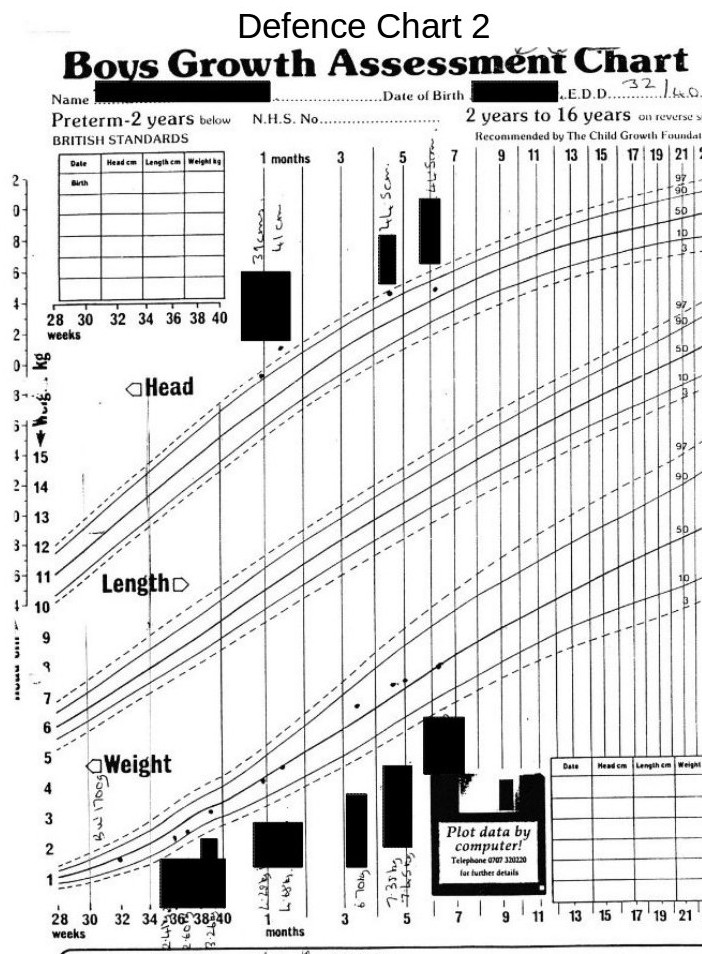
Defence Chart 2
Strange!
Medical Incompetence or Medical Fraud?
The following chart is on produced by someone on the prosecution team and issued to at least some of the medical/surgical experts in the prosecution team. The family received this attached to the back of a copy of a report issued by one of the medical experts.
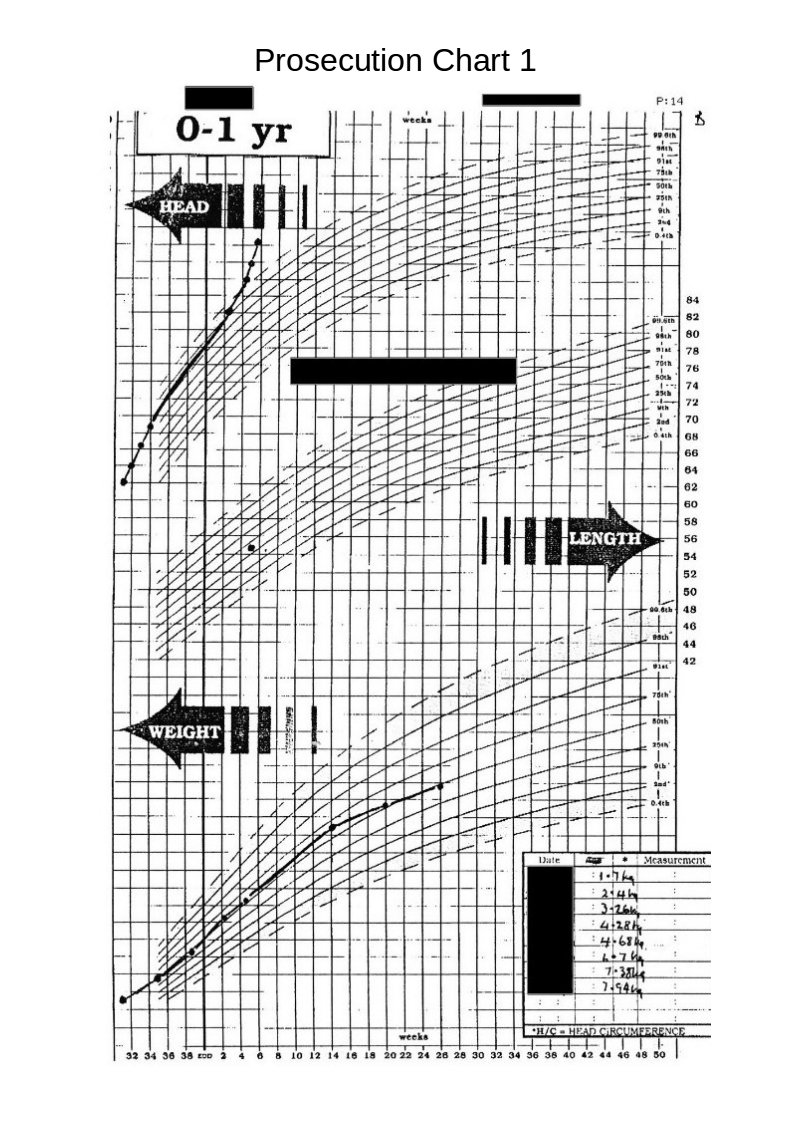
Prosecution Chart 1.
Again we see differences between this and the original charts. The difference between the low weights shown on the original charts and weights shown on this chart, which seem to have mysteriously moved towards the 50th centile, are obviously suspicious.
The head circumference figures (whilst still in hospital), are now lost in a vague area without, any clear definition but indicating that they are on a straight line roughly on the 50th centile.
The following chart, (received with the above chart ) caused me much astonishment and gave me a good, much needed, laugh.
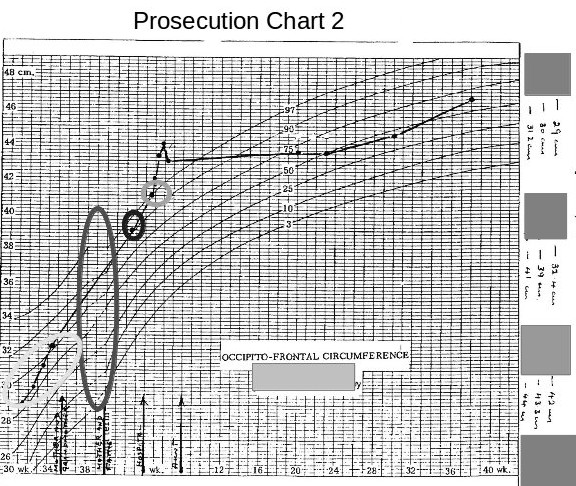 The most obvious thing at first glance was that the chart was a fake made up from two different charts, the long ellipse highlighting the join between the two graphs.
The most obvious thing at first glance was that the chart was a fake made up from two different charts, the long ellipse highlighting the join between the two graphs.
The second most obvious error is that this chart now shows all the head measurements, taken whilst the baby was in hospital, have now magically moved to above the 50th centile. (I would imagine that this is a medical impossibility for a baby being born 9 weeks premature and having a birth weight of 1.7 kilogrammes.)
The third interesting item is that the measurement taken at the health centre and the one taken later at the hospital, have now fallen considerably.
These discrepancies mean whoever produced these charts was grossly incompetent or that these charts produced by the prosecution are deliberate fraud.
Now compare the above chart with the one below.
 This is one of the explanatory charts I produced for the defence report.
This is one of the explanatory charts I produced for the defence report.
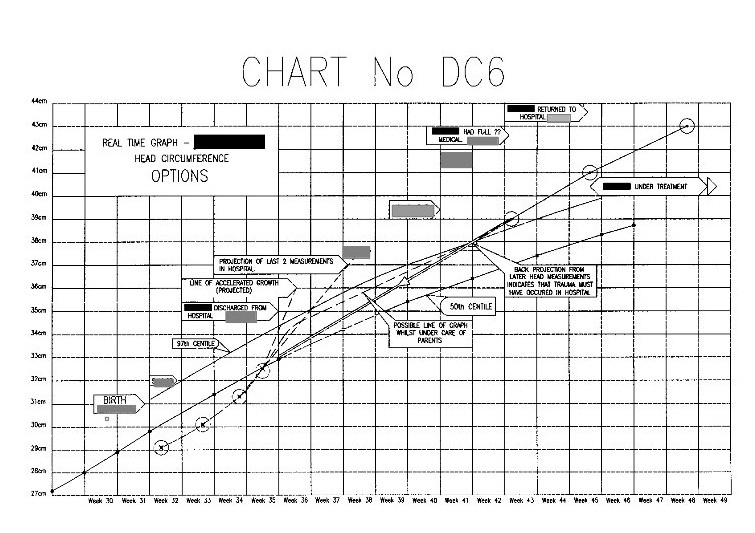
All of the actual seven head measurements taken in this period are in the correct positions relative to the time scale. The horizontal divisions are in weeks, and the vertical divisions are in 1cm intervals.
Obviously it looks totally different from the previous prosecution one.
Let us look closer at this chart.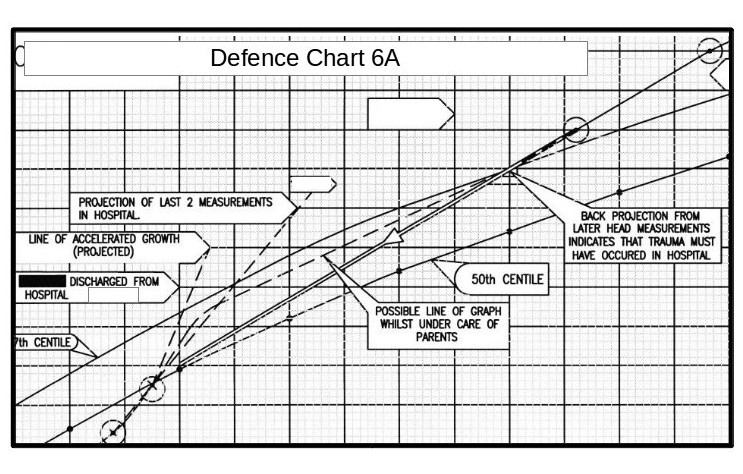 The measurement in the top right hand corner is that taken after the parents took the baby to the doctor and then hospital. The next measurement down is that taken at the Medical Centre two weeks before. All the paediatricians stated that some incident must have happened between these dates (i.e throwing the child about or throwing him onto a hard surface) to account for for the head swelling.
The measurement in the top right hand corner is that taken after the parents took the baby to the doctor and then hospital. The next measurement down is that taken at the Medical Centre two weeks before. All the paediatricians stated that some incident must have happened between these dates (i.e throwing the child about or throwing him onto a hard surface) to account for for the head swelling.
However, projecting a straight line between these these two points backwards, brings it almost exactly to the last measurement made in the hospital.
Author – Brian Williams.
-
Posted on January 24th, 2015
Brian
Shortly before the start of the Court Hearing the Social Services Department (SS) asked the accused parents to attend a meeting with them, to apparently discuss what would happen during the hearing. They were told that they did not need members of their families or legal representation to be present. (NOTE; Prior to this meeting members of the families and/or a legal representative were always present, a condition insisted on by the parents and family.)
It should also be noted that the family had, from May******* onwards, persisted in requesting that the evidence gathered by the family should be read and considered. The request was consistently refused by the SS., stating that all the evidence could only be presented and considered at the trial. Even the “Expert” consultant appointed by the court to represent the parents refused to look at the evidence gathered by the family.
The only none family members with detailed knowledge of this evidence were the family solicitor, (provided by the court), The Guardian-ad-Litem (provided by the Council and representing the child) and myself.
Leading up to this stage, the family had stated on various occasions that they would bring counter-charges against the social services on the grounds of incompetence and failing to carry out their duty to investigate. (This is documented)
During this latest meeting the parents were told that the court hearing would be cancelled if the parents would sign a document absolving the Social Services from any faults. It should be noted that parent’s solicitor and the family were unaware of this meeting until much later.
At this time both the parents were severely stressed and in no state to consider this sensibly and signed the document.
What caused this sudden magnanimity by the Social Services?
As the social services had consistently refused to discuss the evidence, I feel that the Guardian-ad-Litem must have warned them that to take the case to court would cause them serious repercussions.
The Court hearing was cancelled.
Was this the happy ending for the family?
No.
More on this later.
Author – Brian Williams
-
Posted on August 5th, 2013
Brian
What is an ‘Expert Witness’?
Perhaps we should really ask ‘What is an Expert?’.
A genuine expert is someone who knows everything about a particular subject. There are very few subjects that anyone could claim that they know everything about. There are many subjects that very little is known about and therefore no-one can claim to be an expert. I worked with a man who had spent 30 years calculating the settings and other parameters for pressure control valves. In this very narrow field he could be considered to be an expert. ( He did have the unfortunate habit of going to sleep whilst working, still holding his slide rule up in front of his eyes, but totally asleep.)
Would he classified as an expert engineer? Not really, there are thousands of such narrow specialisations possible in engineering, although generally engineers tend to have a wide range of knowledge within engineering and prefer not to specialise because it is boring and reduces your job prospects. (I once interviewed a candidate for a job that needed a reasonable proficiency in steelwork construction. He had worked in the engineering office of a company involved primarily in structural steel for the oil and gas industry. He told me that he had worked for this company for 24 years, producing manufacturing drawings, but then stated that he did not do calculations! I questioned him further on this point and he told me that he had never, ever, done calculations in his job, and wouldn’t know how to start!)
An expert chemist would be able to give you the exact formulation for any substance you required to suit your exact specification. There are no expert chemists. This is not the fault of the chemists, there is so little knowledge available on chemistry. Most chemists are involved in finding knowledge that in the far future may produce ‘An Expert Chemist’.
The same problem applies to biology, both human and animal. We are probably 2000 years away from producing a ‘medical expert’, even just considering human biology. Even this may never happen due to variables caused by the Golden Ratio in biology. (See “Origin of the Golden Section _ Rev 2.”).
Someone could have all the knowledge that is known or has ever been known about a particular subject and yet be essentially ignorant of the subject.
It is essntial that people should be aware of things that they do not know. A child of age five can be forgiven for thinking that he/she is an expert on language after learning to read. By the age of 11 years they should start to understand that they are not experts. At the ages of 15 and 18 there are more shocks for them. At university they start again being ‘dumb kids’ (according to their teachers).
We now come to a further problem. Tuition is about passing knowledge from teacher to student. The knowledge passed on is limited to the knowledge available to the teacher. In subjects like medicine and chemistry there is very little actually known about the subjects. ( If you are a university student you may argue that there is too much to learn already, and you would be correct.) To become expert in these subjects you would spend your whole life at university just covering existing knowledge. But humanity is still at the very beginnings of its knowledge of these subjects. Obviously, we cannot wait a thousand years for an expert to finally come along to solve our medical problems, so we have to guess, keep trying different options etcetera in the hope of finding something that works. This struggle is part of human evolution.
So, when you refer to an expert in medical terms, you are referring to someone who has a very small amount of knowledge of a subject that is colossal in scale.
Over 50 years ago I was suffering from quite severe stress and depression (work related). I finally went to my local chemist. and I was given a quarter pint bottle of a oily looking yellow liquid. I was told to take two tablespoonful per day until I was OK. In three days I was fit and raring to go. I did not have any more of the medicine, nor have I ever needed it since. It was highly effective and was not addictive. Compare this with the £millions spent on addictive drugs that just don’t work for stress and depression patients. This remedy cost me about 6 shillings, a minute fraction of the cost of (non-working) modern equivalents. It should be clear that that the ‘medical experts’ were not actually experts then, nor are they experts now. The same argument must apply to the manufacturers of the high priced ‘non-working’ medicines. I do not know if the medicine I received was a proprietary product or was prepared by the chemist himself.
So what is an “Expert Witness”?
First of all he/she will probably be a ‘specialist’ not an expert. Secondly, the word ‘witness’ means that you have seen and/or examined something.
In a law court an ‘expert witness’ may say that he examined a victim and observed spots on the victims back, or an axe embedded in the victims head, or cyanide in the victims organs. He will be able to supply photographs or test results to prove his statements.
Unfortunately, he is then asked for his opinion on what these results mean. Only ‘expert witnesses’ are ever asked for their opinions, ‘ordinary witnesses’ are banned from expressing opinions.
However, ‘opinions’ should never be considered as evidence. Preconceived ideas affect opinions. An ‘ordinary witness’ may or may not have any preconceived ideas about the evidence, but an ‘expert witness’ almost certainly will. His opinions will generally be governed by the opinions of his teachers and those of the authors of books on his specialist subject, and almost certainly by the current medical ‘fashion’. It wasn’t so long ago that any man visiting the doctor was first asked if he wore tight underpants. If you unfortunately said yes, you were told to go home, buy some new underpants and come back in 6 weeks if that didn’t cure the problem. That is now out of fashion, because I have not been asked that in over ten years.
This is a problem of education. Technical subjects have a fairly intense educational programme that means the student must pass the exams every year. Examination success depends on remembering the information that you have been taught. The student does not have time to analyse what he is being taught, he just has to believe that it is the truth. If he passes all his exams he then starts his career and then for years he does not have time to analyse the validity of what he is practising. (Years ago I often visited hospital accommodation blocks across Britain. In most cases the doctor residents appeared to need medical attention more than the patients they were looking after.)
It is only a few years ago when younger doctors were working over 100 hours per week. This does not leave a lot of time for eating, sleeping, recreation and a love life. It leaves no time for medical research or analysing the work that they do.
The Shaken Baby Syndrome.
Author. Brian Williams
—————————————————-
Further Reading from other sites
The Five Percenters
PO Box 23212 Newcross. SE14 5WB
London
England.
Tel. Number: 020 7639 0942.
email: sbs5@dircon.co.uk
—————————————————-
http://medicalmisdiagnosisresearch.wordpress.com/
——————————————————-
New Research on SBS.PDF
University of Winconsin Law School
Legal Studies Research Paper Series. Paper No. 1195
Shaken Baby Syndrome, Abusive Head Trauma, and Actual Innocence:
Getting it Right
This paper can be downloaded free of charge at;
http://ssm.com/abstract=2048374
-
Posted on October 17th, 2012
Brian
The modern version of the Shaken Baby Syndrome presents some rather novel aspects of the justice system.
1. The accuser is nearly always the main suspect, i.e., the hospital.
2. The accused are nearly always the person or persons least capable of defending themselves.
3. The accused are nearly always prevented from accessing evidence.
4. The so called ‘investigators’ are all part of the prosecution team.
5. No evidence is necessary to obtain a conviction, but evidence is needed to obtain an acquittal.
6. The accused are deemed to be guilty unless proven to be innocent.
Intriguing, isn’t it?
Let us consider the above statements.
1 Most shaken baby cases arise after hospital births. Births are traumatic and cause damage to both child and mother. That this trauma and damage is generally unavoidable does not alter the fact that the hospital were involved with this trauma and damage. Even the ‘real’ indications of Shaken Baby Syndrome (damage to arms and neck) could be caused during the birth process.
Therefore the hospital must be considered to be the prime suspect.
2. A young couple are expecting a happy event. The happy event happens and the couple are deliriously happy. After a few weeks it becomes obvious to the parents that there is something wrong with the baby and they take it to the doctor or to hospital. They are obviously worried. They are then accused by the doctor of deliberately causing injuries to the child. Not accidentally, but deliberately.
The parents are then in a state of shock from which they will never completely recover.
This mental trauma is deliberately caused by people whom the couple trusted implicitly, and is normally a knee jerk reaction from the doctors. Previous medical problems or birth problems are not checked until long after the charges are made.
3. The doctor now informs the Social Services (SS) that he has charged the parents. Any investigation is then supposed to be handled by the SS. However, they no not have any expertise in medical matters, nor do they seem to have any investigation experience. Any experienced investigator would recover/copy all medical records immediately before they can even start an investigation. This never happens with the SS. Months can go by before any records are made available, especially to the defence. Without full medical records the defence cannot begin to prepare their case.
4. The Social Services normally only ‘investigate’ the parents, never do they investigate the doctors or hospital. In general, their investigations actually amount to continuous attempts to get one or other of the parents to confess to shaking the baby. Therefore the SS become part of the prosecution team.
5. Very rarely is evidence pertaining to the cause of the injuries produced in court. The verdict is usually arrived at by vote amongst the medical experts attending the final hearing. The voting is normally split between the paediatric ‘experts’ who vote guilty and various other experts who’s vote can be split.
However, usually the other experts votes are dependant on the information supplied by the paediatrics department of the hospital in which the birth occurred.
6. From the instant that the doctor makes the charge against the parents there are assumed to be guilty. Added to this problem is that the SS department try to insist on secrecy between them and the parents during the claimed ‘investigations’. This normally prevents the parents from obtaining expert help. A further problem is that the defence is prevented from presenting evidence before the court case.
The problem with expert witnesses is that they may arrive at a situation were they ought to vote one way, but doing so would invalidate their decisions in previous cases. Therefore their decision making is affected by their statements made in other cases.
Shaken Baby Syndrome has nothing to do with retinal haemorrhages or brain damage. It is strictly related to damage to the arms and/or neck.
The triad of symptoms currently being claimed by paediatricians to be caused by baby shaking are actually symptoms commonly caused by birth trauma.
Damage to the child’s head during the birth process can cause subdural haematoma that in turn can cause hydrocephalus (brain swelling), which in turn can cause retinal haemorrhages.
What hospitals have done is to take the symptons of the Shaken Baby Syndrome, (which is a sensible, scientific and logical set of symptoms), added in symptoms that are common in child birth, and then deleted the symptoms actually relating to the Shaken Baby Syndrome. Justice or corruption?
See Retinal Haemorrhages on this web site.
Author; Brian Williams.
See also; http://medicalmisdiagnosisresearch.wordpress.com/
-
Posted on April 25th, 2012
Brian
NOTE:- All names and dates have been changed apart from in extracts from medical literature.
RETINAL HAEMORRHAGES.
Consider this extract from ‘CLINICAL EXAMINATION’, page 384. “ The use of the ophthalmoscope is dealt with in Chapter 11. The difficulties of this examination in children are often considerable. To maintain the young child’s gaze in a fixed direction it is usually necessary for a second person to arrange some diversion which for the child has an element of expectancy about it. The examiner, after positioning the patient may say ,’Tell me when the torch flashes’, the torch being held in an appropriate position by a helper who may be mother or nurse, or ‘Tell me how many fingers nurse has up – how many now?,’ the nurse changing the numbers of fingers and thus maintaining the child’s attention. With younger children sedation may be necessary and in certain circumstances even a general anaesthetic may be required.
Extract from Medical Literature.
“They [Retinal haemorrages] are also reported to occur in a percentage of new born infants e.g. 14% in a study by Sezen:(……) and 20% Small(…) who found evidence of retinal haemorrhages but no evidence of intracranial injury on Magnetic Resonance Scanning subsequently. These retinal haemorrhages resolve within a short time after birth e.g. 10 days…….”.
Here is an argument stating that there is evidence of ‘spontaneous’ retinal haemorrhages’ in a significant number of the newly born, but that these normally clear in 10 days.
It is evident from the above extract that retinal haemorrhages are commonly caused by extremely minor ‘trauma’ and are not particularly indicative of a shaking injury.
One should remember that blood circulates by surges in pressure. Restriction of the veins leading away from any part of the body cause excessive pressure surges in that part of the body.
Place an elastic band on a finger or around your wrist and this excessive pressure can be clearly felt in the extremity. This is because the elastic band only restricts the veins carrying blood away from the affected part, but the arterial blood flowing into the hand or finger is not restricted. If the restriction is long lasting then serious damage can be caused to that part of the body. If one considers a blood pressure cuff being gradually inflated over a period of weeks or months, the pressure in the veins will gradually build up until the pressure exerted by the cuff is sufficient to stop the blood flowing. If then left in this state serious damage would be caused.
In regard to retinal haemorrhages, if the veins leading from the eye are restricted, as can happen in hydrocephalus, there can be either a rapid or a gradual reduction in the blood flow. As the veins themselves require blood to sustain themselves in good working order, lack of blood flow weakens them. The areas of the eye being served by the capillaries are also damaged due to lack of blood flow. The increased pressure pulses remain but no fresh blood is being supplied. After a while the weakest veins, i.e. the capillaries in the eye, or the part being supplied, break down due to the increased pressure pulses and the poor condition.
It is evident therefore that there can be no precise time scale for the development of retinal haemorrhages.
My Own Retinal Haemorrhage.
The year following this court case I suffered a retinal haemorrhage.
I was driving out of a city centre when a black spot appeared in my right eye. This quickly changed into a black snakelike shape and then into multiple treelike branches, and finally a deep red haze that completely closed all vision in my right eye.
Luckily, having worked on the above case I immediately understood what had happened. I asked a passer-by for the location of a doctor, and within 20 minutes I was on my way to hospital by ambulance. A week later I had the first laser treatment.
Discussing the problem with the surgeon, she said that I must have an infection or I must have had a bang to my head in the last couple of days. Tests showed no signs of infections, and I certainly had no bangs to my head in the last few days.
However, I did have a severe bang to my head 6 weeks before, when I bent down to stroke our labrador dog who jumped up to lick me at the same time, causing a collision of heads. Both of us ended up on the floor stunned for a few minutes.
For the weeks following, from dusk onwards I was aware of flashing lights in front of my right eye. These continued for the 6 weeks until the retinal haemorrhage occured. I went into hospital for laser treatment for the retinal haemorrhage about a week to 10 days later.
The surgeon was adamant that the dog incident was too early to have caused my retinal haemorrhage, but could not suggest an alternative hypothesis.
Author – Brian Williams
-
Posted on April 15th, 2012
Brian
You will not find much humour in this series of posts. The original report on which it based was produced while I was in a state of anger, over many months, at the lack of honesty and professionalism by the prosecution.
Syndrome – From Google.
- A group of symptoms that consistently occur together or a condition characterized by a set of associated symptoms.
- A characteristic combination of opinions, emotions or behavior.
In the ‘Shaken Baby Syndrome‘ the original symptom responsible for the name was damage done to the upper arms of a baby or child. This could be bruising, breakages or shoulder dislocations, or a combination of these. Later, in some cases, damage was discovered to the child’s neck. These symptoms should normally lead to the suspicion of Shaken Baby Syndrome.
This type of injury is not, in itself, proof of the baby being shaken. Some-one catching a falling child could accidentally inflict the same injuries. Bruising on one side of one arm alone would indicate the possibilty of a falling injury.
A falling child could suffer a single arm bruising, neck injury and broken arm. A child falling downstairs could have all of the above injuries.
Neck injuries without damage to the upper arms should indicate that ‘Shaken Baby Syndrome’ does not apply.
‘None shaking’ neck injuries would show bruising or cuts to the head or neck.
Now consider the following extract from Google
Shaken baby syndrome (SBS) is a triad of medical symptoms: subdural haematoma, retinal hemorrhage, and brain swelling from which doctors, consistent with current medical understanding, infer child abuse caused by intentional shaking. In a majority of cases there is no visible sign of external trauma.
SBS is often fatal and can cause severe brain damage, resulting in lifelong disability. Estimated death rates (mortality) among infants with SBS range from 15% to 38%; the median is 20%–25%. Up to half of deaths related to child abuse are reportedly due to shaken baby syndrome. Nonfatal consequences of SBS include varying degrees of visual impairment (including blindness), motor impairment (e.g. cerebral palsy) and cognitive impairments.
Notice the complete lack of any mention of arm injuries or neck injuries.
A few years ago I was requested to carry out an investigation into the medical evidence presented by the prosecution in a case claiming that the parents had caused life threatening injuries to their infant son by seriously shaking him and throwing onto the floor or onto a hard object.
The prosecution team (against the parents) included 12 consultants and 6 Social Services personnel. The defense team proposed by the Social Services, comprised the parents, an inexperienced solicitor and a medical consultant who was later revealed as a professional prosecution witness in this type of case. (The social Services admitted that they had to work in accordance the charges, and spent most of their time attempting to get the parents to admit their guilt.) The parents had been told by the Social Services that they must not tell any-one about what was happening, but the parents had more sense and told their parents.
The family then decided that they would have to handle the defense themselves, and began collecting published medical information. I became involved when I was asked to draft a letter for them repudiating some legal point.
After many months I did manage to prove that the parents were not guilty, and that the damage occurred at the hospital.
What was the damage?
Subdural haematomas.
Retinal Haemorrhages.
Brain Swelling.
So we had the situation that the child had all the symptoms claimed by the prosecution to prove ‘Shaken Baby Syndrome, but I could prove that the damage actually occurred at the hospital. This throws the validity of all the evidence required for justification of ‘shaken baby’ trials into serious doubt.
The interesting point about all this is that the prosecution was instigated and controlled by the people responsible for the injuries
The medical use of the Shaken Baby Syndrome has become a ( as stated under Syndrome – category 2),
“A characteristic combination of opinions, emotions or behavior.”
Unfortunately this relates to medical professionals, not patients.
If you or anyone known to you is accused of ‘Shaken Baby Syndrome’, get a solicitor or lawyer to insist on the immediate release of copies of all medical records relating to the child.
In this particular case the first item of the medical records was accidentally received by the defense 5.5 months after the charges were made, despite repeated request for full records. Some items presented to the court by the prosecution were forgeries.
Author – Brian Williams – Contact e-mail —nets@talktalk.net
Additional Reading.
The Five Percenters
PO Box 23212
Newcross SE14 5WB
London
England.
Telephone Number: 020 7639 0942
email: sbs5@dircon.co.uk.
Web Sit:sbs5.dircon.co.uk
-