

-
Tin, BPA, BPS and Phthalates.
Posted on July 19th, 2015 No commentsA Preliminary Investigation into My Death. See also “boil or carbuncle” .
At the present time I am dying due to continuous carbuncles that are effecting the operation of my normal bodily processes. In the last eight years there has rarely been periods of longer than 5 to 6 weeks that I have not been suffering from an active carbuncle.
At present (14th July 2015) I am suffering from a carbuncle in an awkward position on by backside. This is in its (I hope) final stage after 5 weeks continuous leaking. (Update; 10th September 2015. I am still having to change dressings twice a day, so no improvement yet.)
The medical profession claim these carbuncles are boils and insist on prescribing antibiotics that have no effect on the problems.
They claim that boils and carbuncles (and furunculea) are all the same thing. THEY ARE NOT. See “boil or carbuncle“.
60 years ago I learned that carbuncles are not caused by streptococci. Boils are caused by streptococci. This was a simple experiment. Having had a carbuncle two years before, when I had a painful, throbbing boil erupt on my neck I decided to try stannous oxide tablets, as these had an almost miraculous healing effect on the earlier carbuncle after months of injections and capsules of antibiotics provided by the medical ‘experts’. Stannous oxide tablets had no effect on the boil. Chemists knew there was a difference between carbuncles and boils but the medical profession did not and still refuse to accept that there is a difference.
Is this criminal negligence by the medical profession? In one way it is. The refusal of (or inability) of medical personnel to listen to patients is a serious problem. I have never had any doctor ask me whether the prescriptions he issued to me actually worked.
Some prescription medicines include questions about side effects. Is the fact that the medicine prescribed has no effect on the complaint or illness and therefore extends the duration of the problem, not a side effect?
I have recently obtained 20 grammes of Tin that I trying to purify sufficiently to pass my own safety requirements. This will probably take a few weeks. Note; I will still have the problem of determining whether the tin or the oxide is the crucial component: I feel that the oxide is the most likely but I hope that my body can create the oxide.
Update 6th April 2016. I am convinced that my body can handle handle the tin and use it for my benefit, however, I feel that tin oxide (Sn(ll) itself is providing the improvement and that oxygen in the blood is modifying a small proportion of the tin into SnO. Tin metal itself is not a natural substance.
******************************
Ongoing notes relating my current attempt to self medicate.
- At present (4th October 2015). Over the last two weeks I have been taking approximately 200 milligrams each day of tin powder. (Note this is now correct, there was a fault on my electronic weighing unit)
- Over this period I have noted the following; Swellings under both my arms have almost disappeared (after about 8 years). Pubic and underarm hair growth has increased. (But I am still going bald.) Over the last three days leakage from my current carbuncle has almost stopped. PLUS (relating to type 2 diabetes) sensitivity on the soles of my feet has improved, making walking a lot easier. It is obviously too early to get excited about these improvements. I will continue with the low dosage because I am still not confident about the quantity of contaminants. However, it does seem that by my body can use the tin itself.
- From the 1st of October 2015 I have rather complicated this series of tests by stopping taking statins. This was because it has been claimed by many sources that statins can cause leg muscle problems, which I have suffered from for about 18 months. Over the last two weeks I have noticed a significant improvement in my walking ability. A further unexpected result is a complete stoppage to my falling asleep at odd times during the day, often for 2 – 3 hours. I have not fallen asleep even once during the day since the 1st October.
- 1st December. Still not dosing off during the day. Carbuncle leakage stopped. No further improvement in walking.
Brian,
*****************************
It is only recently that I have looked into the background to the changeover to plastic lined tins. I naturally assumed that it was just to make more profits for the involved companies. However, I find that not only that the companies have effectively prevented access to a highly beneficial vital mineral (SnO), they have replaced it with a toxic alternative.
—————————————–
NOTE: I have used lots of information from the ACU-CELL website (http://www.acu-cell.com/) which I have found interesting, well written and logical. However, I have still not found their address so that I can write to them.
“Health Benefits & Toxicity of the Element Tin, and its Effect on Adrenals, Depression and Fatigue. Copyright © 2000-2015 Acu-Cell – Tin – Health Effects.
While Tin (Sn) has been established to be an essential trace element for some animals (they won’t grow well without it), some researchers are still unsure of whether tin is essential to human health. Daily dietary intake of tin from various food sources is in the 1 – 3 mg range, which is less than 1/10th of the daily intake obtained years ago before lacquering tin cans, switching to aluminum cans, or, in the more distant past, when tin cups or tin pans were still in use. Since bronze contains copper and tin, the use of tin has been established well past the Bronze Age, several thousand years ago.Rat studies have shown that tin-deficient diets resulted in poor growth, reduced feeding efficiency, hearing loss, and bilateral (male pattern) hair loss.”
“Tipton and Shafer examined tin in human tissue after accidental deaths.
They noted that tin was found in the aorta, brain, heart, kidney, liver, muscle, ovary, spleen, pancreas, testes, stomach, and uterus, but none was found in the thyroid of any victim, while the prostate, which usually shows no other trace element, had tin.”
[Note by Brian; Since the canning industry stopped the use of tin only and replacing the tin with a BPA lining I have had Pancreitus , Heart problems including a triple bypass and Prostate cancer.]
“Average concentrations were the same range as cobalt, iodine, chromium, and selenium, which are known vital nutrients. Inorganic tin is capable of entering into biological activity at saline pH, and it is far less toxic than other known vital trace elements such as copper and cobalt. In addition, tin levels do not vary statistically with age, gender, or geographical areas. Misk found traces of tin in the fetal heart and spleen, and higher levels in the liver, while Schroeder and others reported no tin in stillborns.”
Tin is associated with Iodine the same way as calcium is associated with magnesium (see “Tin & Iodine” for details). Tin supports the adrenal glands, and iodine supports the thyroid gland, with both subsequently affecting cardiac output: Tin + adrenals control the left side, and iodine + thyroid control the right side. In addition to low Vitamin C and/or Vitamin B1, low tin is a common nutritional cause of low adrenals, which can lead to left-sided cardiac insufficiency. While fatigue or depression may be experienced with cardiac insufficiency of either side, breathing difficulties or asthma are more common with left-sided cardiac insufficiency, and swelling of hands and feet is more common with right-sided cardiac insufficiency,regardless of the cause.Comparing thousands of patient records showed that better than 90% of patients tested exhibited moderately low, to very low levels of Tin when referenced to the status of all other essential trace minerals, making tin the most deficient element compared to any other trace mineral measured.I had 285 individuals taking part in the Nutritional evaluation of Tin, some on a short-term basis (3 weeks),and others on a long-term basis (1 – 2+ years), resulting in some valuable feedback on various responses encountered, including side effects, although the rather poor absorption of stannous oxide was a limiting factor in being able to achieve optimal cellular levels of tin in all subjects.Of the changes experienced after supplementing tin, negative reactions, e.g. stomach / digestive upsets, or skin reactions, were at par or less compared to the best tolerated trace minerals such as chromium, calcium, or magnesium. Positive health effects were numerous and included improvements with fatigue, some forms of depression, and a general increase in energy, well-being, and mood. There were also benefits with certain types of headaches, insomnia, asthma, or improvements with digestion, skin, or various aches and pains.Tin poisoning (https://en.wikipedia.org/wiki/Tin_poisoning)
Main article: Tin poisoning
Tin poisoning refers to the toxic effects of tin and its compounds. Cases of poisoning from tin metal, its oxides, and its salts are “almost unknown”; on the other hand certain organotin compounds ( https://en.wikipedia.org/wiki/Organotin_chemistry#Toxicity} are almost as toxic as cyanide.[25]
—————————————-
Extract from;
IBISWorld UK. UK Industry Market Research: Data & Analysis on 400 Industries.
www.ibisworld.co.uk.
What Kind of Cans Are Used for Canned Foods?
by Bonnie Singleton, Demand Media.
The majority of cans used for canned foods around the world today are made from steel. Although there is a thin layer of tin on the surface, there is only 5 to 6 pounds of tin per one ton of steel used.
Canned Controversies.
Almost all metal food and beverage cans contain an industrial chemical called bisphenol A, or BPA. The chemical is used in epoxy resins that coat the inside of food cans. There is a growing concern from scientists and health organizations like MayoClinic.com that BPA can seep into food or beverages. This is a problem because BPA has been linked to prostate and breast cancer, heart disease and damage to the prostate gland of fetuses, infants and children. To avoid this danger, look for cans labeled BPA-free.
But,
BPA vs. BPS Options
Cans need to be lined with something, and you’ll typically have no way of knowing what that “something” is. Often, it’s a similar chemical known as bisphenol-S (BPS).
Unfortunately, BPS is not a safe alternative. Research has shown BPS has estrogenic activity comparable to estradiol, the most potent human estrogen. It was also found to be capable of enhancing estradiol-mediated cell signaling, making it a particularly potent endocrine disruptor.6
Furthermore, the study showed BPS can induce apoptosis (cell death) and interfere with cellular secretion of prolactin (PRL)—a hormone that regulates hundreds of biological functions, including metabolism, reproduction, and lactation.
Originally, BPS was heralded as a suitable alternative because it appeared to be less prone to leaching than BPA… but it must be getting into food because the majority of Americans already have detectable levels in their bodies. Scientific American noted:7
“BPS was a favored replacement because it was thought to be more resistant to leaching. If people consumed less of the chemical, the idea went, it would not cause any or only minimal harm. Yet BPS is getting out. Nearly 81 percent of Americans have detectable levels of BPS in their urine. And once it enters the body it can affect cells in ways that parallel BPA.”
Unfortunately, even if a can (or plastic product) is labeled BPA-free, you can’t be sure it’s also free of BPS. And even if it doesn’t contain BPS, there’s a good chance it contains other harmful chemicals, like phthalates.
Banning BPS will not solve this problem, as there are many types of bisphenols, and simply switching from one to another is nothing but a game of toxic musical chairs.
At present, you may be paying more for a “BPA-free” product that is no safer than the old BPA-containing variety… You’re also exposed to a number of other chemicals courtesy of food and beverage containers, most of which have no warning labels at all.
————-
Fluoridation of water supplies.
More information on this at; http://articles.mercola.com/sites/articles/archive/2015/06/20/fluoride-deception-continues.aspx
This is something that I was aware of at the time that the government decided to add fluoride to public water supplies. Working in the chemical industry it was common knowledge that it was very toxic and was difficult to dispose of. Luckily, our local water company refused to add fluoride to its water supplies. However I have since avoided any products containing fluoride, and advised others to do the same. Obviously I cannot argue that fluoride has effected my health.
Stannous Oxide to replace Fluoride in toothpaste?
Extract from “Tin Based anti-Tumour Drugs”, Edited by Marcel Gielen.
Springer Science & Business Media, 29 Jun 2013. (Page 148+)
A traditional belief that the tin workers in Beauve never suffered from furunculosis led to the use of tin and its compounds in the treatment of staphyloccol infections. In 1917 Frouin and Greigore published a study which suggested that tin, tin oxide, stannous chloride and sodium stannate modified the virulence of staphylocci.
[A traditional belief? Or actual knowledge? A furuncula is a carbuncle and carbuncles are not caused by staphyloccol infection. Brian]
This work, based on seven infected rabbits and two control animals, has since been discredited and more recent evidence indicates that neither soluble nor insoluble tin compound of tin have any effect on staphyloccci in vitro or in vivo.
[I personally discovered this in 1956. The work by Fruouin & Greigore I would assume related to transferring infections from a sufferer of a Furuncula (carbuncle) to the host rabbits. If later tests used infection from a boil or stock staphylocci then obviously no effect would be found. Brian]
Nevertheless, the belief that tin had some value in the control of cutaneous sepsis persisted well into the 20th century and resulted in an occurrence of organotin poisoning in France 1954.
[The belief was that tin was valuable in curing carbuncles/furuncles, NOT cutaneous sepsis. This belief was NOT the cause of the organotin poisoning, which was caused by manufacturing negligence. Brian]
The proprietary compound involved, “Stalinon”, had been contaminated with triethyltin impurities and this resulted in the deaths of more than 100 people.
[This is a different type of belief. This belief was by the medical profession, Cutaneous Sepsis does not apply to carbuncles because the sepsis generally starts in the muscles or fat and it can take many days, even weeks for any signs to appear in the cutaneous layer (Skin) Brian.]
In the UK a preparation containing methyl stannic iodide, “Staniform”, was available before 1958 as an external treatment for staphyloccal infections and an oral treatment containing tin powder and tin(II) oxide “Stannoxyl” was available until recently.
[‘Stannoxyl’ was the last treatment I managed to obtain and was old stock in 1984. At the time I was being treated with antibiotics for weeks with absolutely no effect. A local chemist managed to find a single course of Stannoxyl from wholesalers and within a few days I was cured. Brian]
In contrast to the organotins, metallic tin and inorganic compounds are generally non-toxic with the notable exception of stannane, Sn H4, which is more toxic than arsine.
For many years, stannous compounds have been used in dentistry and oral hygiene. As long ago as 1947, it was known that tin(II) fluoride protected dental enamel from dissolution in lactic acid and since then SnF2 has been incorporated into dentifrices, mouthwashes, topical solutions and occasionally. dental cements.
[In 1945 US started adding fluoride to public water supplies. ]
The compound appears to exert its prophylactic and therapeutic effects in several ways. In combination with acidulated phosphofluoride it allows control of dental caries; it inhibits dental plaque growth; it effectively controls root hypersensitivity; it reduces root surface solubility and finally, it causes less mottling than sodium fluoride.
It has been said that the clinical effect of antimicrobial agents as plaque growth suppressors is not well correlated with in vitro antimicrobial assays of the same agents.
Reports indicate that while both stannous chloride and stannous fluoride possess bacteriostatic effects on oral micro-organisms in-vitro [Laboratory tests outside the body], growth inhibition by SnCl2 in-vivo [actual tests in the body] is only slight. However, no explanation has been offered for these different effects and the results may prove to be anomalies caused by the experimental difficulty in keeping stannous ions in solution.
It has been shown that commercial toothpastes containing SnF2 alone or in combination with Tin(II) pyrophosphate (Sn2P2O7), function as efficient plaque inhibitors and it appears that the Tin(II) [Stannous Oxide] ion is the bacteriostatic agent, with little, if any, effect from the fluoride component. Most of the tin retained in the mouth is bound to the epithelial surfaces, the dental plaque and salivary macromolecules and is slowly released over a period of about 4 hours following brushing, thus allowing a long lasting bacteriostatic effect.
[Therefore there is no excuse for using fluoride in water supplies, toothpaste or mouthwashes.]
Stannous oxide (Tin(II)) is the safest of all the metallic oxides. Aluminium, Copper, Iron, Cromium, manganese, Zinc etcetera can all become toxic outside of certain narrow limits, whereas Stannous Oxide can be overdosed by a large amount with the only symptoms being similar to eating too many apples.
Brian.
———————————-
Essential Minerals
The fact that Tin is not deemed to be an essential mineral is, I feel, due to poor experimental practices. I will explain some of these later.
My main purpose at present is to solve my problem of severe tin shortage in my diet. Normal dietary input is limited to 1-3mg per day against a recommended figure of 10-20mg proposed by Acu-Cell. (Note: Acu-Cell don’t seem to want to sell you any supplements and give no advise on how to get them. I’ve tried)
Most of this is not retained in the body. Adding to this problem are ‘antagonists’, chemicals that reduce the effectiveness of the tin that is retained in the body.
In the Chart below (From Acu-Cell) the blue line indicates the ‘Normal’ for healthy people. Note; The Normal line does not mean that the same amounts (mg) are involved. ‘Normal’ for one element may be 10mg but normal for another element may be 1000mg.
Note; You cannot just increase one item and hope for a cure. A careful balancing is required between multiple elements. You need to go to the Acu-Cell website for much further information.
Brian
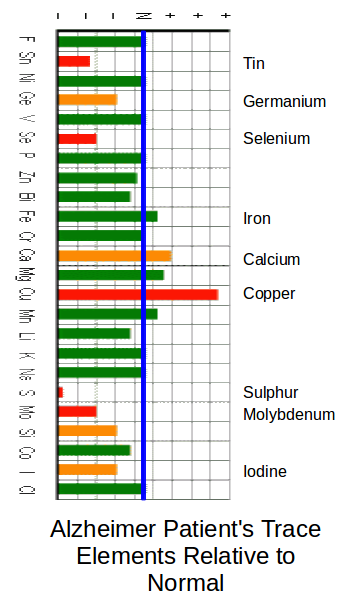
In this chart three of the main Tin antagonists are at above normal levels: These are Iron, Calcium and Copper.
Low levels of Tin and Iodine would indicate that there would be some heart efficiency problems.
Low levels of Selenium and Germanium would indicate some brain and nerve problems.
Low levels of Selenium and Sulphur can indicate a wide range of problems including Arthritis and nerve problems.
Note; The extremely low sulphur levels in Alzheimer sufferers tends to highlight a set of problems for the elderly. Egg Yoke is the main natural source of sulphur. Egg Albumin (The White of Egg.) apparently causes constipation in the elderly. Recent medical opinion advises people to eat less eggs. Carers tend not to give eggs to the elderly due to the constipation problem.
—————————————–
Phthalates What are they and What are their dangers?
© 2015 Guardian News and Media Limited or its affiliated companies. All rights reserved.
Phthalates are everywhere, and the health risks are worrying. How bad are they really?
Phthalates are everywhere, and a tidal wave of new research has documented their wide-ranging negative health impacts, but what are the real risks?
Lately, it seems like a new study on the health impacts of phthalates comes out every week. The chemicals are everywhere: they’re used in everything from household cleaners to food packaging to fragrance, cosmetics, and personal-care products.
In 2003, researchers at the US Center for Disease Control documented widespread exposure to a high level of a group of chemicals called phthalates (pdf) across the general American public. The chemicals act as binding agents and also make plastics flexible.
The CDC recommended that the chemicals and their effect on human health be studied further, a recommendation that helped unlock funding for dozens of studies focused on phthalates, resulting in a tidal wave of recently published reports that largely indicate the CDC’s concern was warranted.
The CDC’s warning on phthalates also caught the attention of senators Barbara Boxer and former US representative Henry Waxman, who included the class of chemicals in their Consumer Product Safety bill, passed in 2008. That bill banned the use of some phthalates in children’s products, passed an interim ban on others, and required that the Consumer Product Safety Commission take a close look at the chemicals.
While phthalates is a huge class of chemicals, several have been shown to have negative health impacts.
The resulting report on phthalates – the Chronic Hazard Advisory Panel (Chap) on Phthalates (pdf) – was finalized in late 2014, and despite the chemical industry’s efforts to soften the commission’s recommendations, public health advocates are largely pleased with the effort, a rarity when it comes to government-penned reports on chemical safety.
With academic studies and policy reports consistently voicing concern over the health impacts of phthalates, and consumers beginning to sit up and take notice, regulation may not be far behind.
“The Chap report is the first major regulatory document in the federal government that’s highlighting the extent of the new science on the risks of phthalates,” says Erik Olson, senior strategic director of food and agriculture and health programs for the Natural Resources Defense Council. “The fact that the commission is looking both at phthalates as a group and at the toxicology of individual phthalates is really important,” he says.
Olson was the deputy staff director for the US Senate’s environment and public works committee when the Consumer Product Safety Bill was written and passed. Between the Chap report, a National Academy of Sciences report looking at phthalates as a class and what he calls “the tidal wave of research that’s been coming out fast and furious” in the past year or so, he said, “we’re getting past the phase of complete denial from the industry – they can no longer claim that there’s no risk at all with phthalates.”
What’s the harm?
Name a major public health concern over the past two decades and there’s likely some link to phthalates exposure.
In the past few years, researchers have linked phthalates to asthma, attention-deficit hyperactivity disorder, breast cancer, obesity and type II diabetes, low IQ, neurodevelopmental issues, behavioral issues, autism spectrum disorders, altered reproductive development and male fertility issues.
While phthalates is a huge class of chemicals and nowhere near every chemical in the class has been studied, several have been shown to have negative health impacts: butyl benzyl phthalate (BBzP), dibutyl phthalate (DnBP), di-2-ethylhexyl phthalate (DEHP), diethyl phthalate (DEP), di-butyl phthalate (DBP), benzyl butyl phthalate (BBP), diisobutyl phthalate (DiBP), diisononyl phthalate (DiNP), di-n-octyl phthalate (DnOP), dipentyl phthalate (DPP), di-isobutyl phthalate (DiBP), di-isononyl phthalate (DiNP), di-n-octyl phthalate (DnOP), di-isohexyl phthalate, dicyclohexyl phthalate (DcHP), and di-isoheptyl phthalate.
Enough distinct phthalates have been studied to indicate that companies should proceed with caution when using any chemical in the phthalate class, particularly in products for pregnant women or young children, whom the research has indicated are the most vulnerable to the effects of phthalates.
One of the first phthalates to raise a red flag, DEHP, was replaced in hundreds of consumer products with DiNP, only for researchers to discover a few years later that exposure to DiNP is correlated to male genital birth defects and impaired reproductive function in adult males.
Public health advocates hope to learn from the mistakes made in regulating bisphenol A (BPA) as momentum gathers behind the regulation of phthalates, and ensure that one harmful phthalate isn’t just replaced with another over and over again.
BPA was singled out as the sole chemical of concern in the bisphenol group, and regulated as such. Manufacturers largely replaced BPA with bisphenol S (BPS), which researchers are now discovering is equally as problematic as BPA.
With phthalates, the research has come before any sort of regulation – companies are not even required to list phthalates on consumer product labels – and legislators are already looking at the entire class of chemicals, as well as any particularly bad ones.
No escape
Both because of their ubiquitous usage and because they are not listed on product labels, phthalates are next to impossible to avoid. They are in household items (vinyl flooring), personal care products (hair care, body wash, some cosmetics), fragrance, household cleaners, and food. Even for those who either avoid these products or buy phthalate-free variations, phthalates lurk in unexpected places.
In food, for example, even milk packaged in glass may have passed through plastic tubes on its way from the cow to the bottle, taking DEHP along with it. “Milking machines use a lot of plastic and DEHP is free and very lipophilic (fat soluble), and milk is full of lipids, so it just pulls the DEHP out of the plastic tubing and into the milk,” explains Robin Whyatt, professor of environmental health sciences at the Columbia University Medical Center and the lead author on several landmark phthalate studies. “So my guess would be that milk is a pretty important source of dietary exposure to DEHP.”
Spices are another surprising source of phthalate exposure. A 2013 study, published in the journal Nature, compared the phthalate levels of two groups, one eating their regular diet but armed with a handout of recommendations for ways to reduce BPA and phthalate exposure in their diet, and the other eating a catered diet consisting solely of local, organic fare, none of which had touched plastic packaging. The study authors were shocked to find that DEHP levels in the local, organic group jumped 2,377% over the course of the experiment. Determined to figure out why, the researchers tested all of the foods consumed by the group and found high levels of the phthalate in dairy products and various organic, imported spices.
“The fact is you can’t know if a food has phthalates in it – you can suspect, but it’s almost impossible to know,” Olson says. “That makes them hard to avoid, which is why you need a regulatory framework.”
What now?
Regulation of consumer products moves slowly in the US, and that has proven to be especially true when it comes to chemicals. Despite the recent movement on phthalates, Olson says it is likely to be a long time before we have the sort of wide-reaching framework that would adequately protect the public from harmful exposure.
That doesn’t mean all is lost in the meantime. State and federal regulations have already eliminated the chemicals from some products, and that list is likely to grow. California’s Proposition 65 now includes four phthalates – DINP, DEHP, DBP and BBP – under its labeling requirements, and the state’s Office of Environmental Health Hazard Assessment (OEHHA) recently proposed changes to Prop 65’s warning requirements, which would require manufacturers to list specific chemicals in their warnings and make those warnings more detailed (currently the warnings are vague, stating only “this product [or building] contains substances known by the state of California to cause cancer”).
“Prop 65 will be a driving force for change on phthalates,” Olson says. “Companies don’t like to put warning labels on their products.”
Consumers can also take matters into their own hands by avoiding products packaged in “recycling-code-3” plastic, products that include the vague ingredient “fragrance” on their label, and purchasing organic products packaged in glass as much as possible.
Whyatt also recommends that consumers remove any food packaged in plastic from its packaging and place them in glass. “DEHP continues to leech over time, so you do actually reduce exposure by changing the storage container, even if it’s been in plastic before you bought it,” she says. “All the DEHP has probably not come out yet by the time you get it home. And if there’s still DEHP in there, it’s probably still leeching out, so you can at least reduce your exposure some extent.”
“If we start by addressing the products where we know there’s significant exposure to phthalates, and we start with the most vulnerable communities – pregnant women and children – we can make a real difference,” Olson said. “We could take care of a lot of food exposure through FDA regulation and toys through the Consumer Product Safety Commission, and that’s a lot. It’s not all, but it’s a good chunk.”
Retailers could also play a significant role, as they have with other chemicals of concern. Target and Walmart both launched initiatives to reduce or eliminate toxic chemicals from their shelves last year. Both retailers have said they will make evidence-based purchasing decisions to protect their customers’ health. With a mountain of scientific evidence piling up on phthalates, it can’t be long before consumers begin to put pressure on retailers and retailers in turn push their suppliers to find both alternatives to phthalates and ways to remove the chemicals from their products altogether.
Phthalates can fairly simply be removed altogether from products, with no replacement, according to “green” chemist Bruce Akers. It’s when the chemicals are used to create tubing or packaging that eliminating them becomes tougher: “If you want soft, squeezable plastic, you’re using phthalates,” Akers says.
But according to Whyatt, companies could be using flexible polymers instead. “There are flexible polymers that don’t require a plasticizer – they exist,” she says. “They haven’t been studied really, so we need to know more, but they probably do not leech the way phthalates do. The problem with phthalates as plasticizers is that they’re free floating, they don’t attach to the polymer, so they leech easily. If you have a flexible polymer that shouldn’t happen.”
Despite the size of the issue, Olson remains positive. “We’ve turned a corner on the regulation of phthalates,” he says. “They’re extremely widely used in the economy and it won’t be overnight that we’ll see widespread phase-outs, but clearly we’ve crossed the river and we’re now at the point of debating exactly which uses need to go and where we can use alternatives.”
Correction: This article was updated on 11 February to say Henry Waxman is a former US representative and not a current senator.
© 2015 Guardian News and Media Limited or its affiliated companies. All rights reserved.
More to follow.
———————————–
This is ongoing research in an attempt to save my own life. It may already be too late, but stannous oxide would stop the carbuncle problem within a few days, [See Boil or Carbuncle.] and allow other aspects of my health to improve.
Author; Brian Williams
- At present (4th October 2015). Over the last two weeks I have been taking approximately 200 milligrams each day of tin powder. (Note this is now correct, there was a fault on my electronic weighing unit)
-
Boil or Carbuncle?
Posted on October 14th, 2010 No commentsIS IT A BOIL OR IS IT A CARBUNCLE?
Summary of differences. Boil,- Painful and throbbing from first day.
- A head will be evident at the infection site on a boil.
- Bursting the head on a boil will relieve the pain.
- Bursting the Head will release pus from the centre of the boil
- The pus leakage will be followed by blood leakage.
- After bleeding stops, healing starts.
- Penicillin, antibiotics will rapidly cure the problem if needed.
- Boils may have multiple heads.
- No throbbing or pain.
- No head visible for a few days or even weeks.
- Swelling in the general area.
- Tapping on the head of the carbuncle when it forms gives a burning sensation.
- When carbuncle bursts, pus leaks out around a central jelly-like core.
- Leakage of pus and blood may continue for weeks or months.
- Penicillin/antibiotics have no curative affect.
- I have never had a multi-headed carbuncle.
- The pus from a carbuncle has a distinctive smell (Stink).
Finally my mother told me to go our local chemist who had a very good reputation. After telling him the whole sad story, he said that he needed to check exactly what is was and then removed the bandages. On revealing the ‘boil’ he immediately said that it was not a boil, but a carbuncle.
He also said that it was easily treated!
He then went around to the back of the shop and returned a few minutes later with a small bottle containing lots of small grey pills.
It cost me 2 shillings (10 new pence). That included supplying his own bottle, the label, his time spent on examinations and profit.
He told me to take all the tablets according to the instructions, and to return when the swelling had gone down.The following morning the swelling had reduced considerably, and by the third day all the swelling had gone, just leaving the original ‘boil’.
Re-examination by the chemist revealed a 1″ diameter open wound with 3/4″ diameter yellow core of Jelly like consistency, which he immediately dug out with some difficulty.
By the end of the week the only sign of the carbuncle was a small scar, which I still have.
What did I learn from our local chemist about carbuncles?
Most of the knowledge about carbuncles came from experiences in the two world wars. He did say that the ‘Multi-headed boil’ description was false and that carbuncles could be single or multi-headed. (I managed to work out why later.)
I have had many carbuncles over the years. One possible reason is that I am susceptible to them. The main reason is that in the early days I got them by being in the wrong place, which is old attics. During the First World War many British soldiers were fighting in old houses and other buildings, many of which were severely damaged. They were covered in the dust from attics and roofs. and quickly infected with boils and/or carbuncles. In the Second World War people in bomb damaged areas were infected with boils and/or carbuncles.
Before this carbuncles were not unknown, but were considered to be just another type of boil, the main difference being that in many cases the carbuncles proved to be fatal.
The first five times I got them after doing work in old attics. but these were rapidly cured without much bother by stannous oxide tablets. Since then I have been unable to obtain the necessary remedy and so have had to go through months of aggravation, changing dressings 2/3 times a day. My last one (about 8 years ago) lasted 16 months and cost me £100’s in dressings plus £100’s in subsidised antibiotics plus continual supplies of vitamin supplements.
Update 30th October 2011. My latest one, started late September 2010 (under my right arm) has now been with me for 13 months. This is probably the one that will kill me, due to my age.
Up date March 11th 2015. The one under my right arm is still with me (3 years and 5 months) One in my groin area has reactivated. At my last of 3 visits to ‘experts’ at local hospital 5-6 months ago, I was told that “….it doesn’t matter what you call it , you can only have antibiotics”. This from the senior consultant.
How to Identify a Carbuncle.
Simplest and quickest test is just to tap on it with your finger. If there is a sharp pain it is probably a boil. If it gives a burning sensation, similar to that caused by holding a cigarette end close to the skin, it is almost certainly a carbuncle.
Carbuncle: [L. carbunculus, dim. of carbo, a live coal, a carbuncle]
Source: Stedman’s Medical Spellchecker, © 2006 Lippincott Williams & Wilkins. All rights reserved.
You would think that this would give a clue to the medical profession!!!
A boil is nearly always more painful than a carbuncle. This is one of the reasons for the ‘multi-headed boil’ problem. You can have a carbuncle for many days without realising it, but a boil makes its present felt immediately. A carbuncle can reach the bursting stage before you become aware of it. When a carbuncle bursts the infection gets smeared across the skin which then creates more ‘heads’. The human body creates a protective film around the site of a boil or carbuncle to prevent the infection spreading and to confine the ‘safety valve’ nature of it to one location. If any of the infected pus from a carbuncle is smeared outside this protected area, new carbuncles start. Contact with this pus can start infections in healthy people, as happened once with my wife. (Luckily for me, the cure was still available at this time.)
If the first infection head is properly ‘dressed’, further heads are prevented. Note; I was advised to do this by the chemist. I personally have never had a multi-headed carbuncle. I have had multi-headed boils.
A second identifier is that boils ‘throb’, carbuncles don’t, another reason why they get ignored.
A third identifier for carbuncles is the ‘core’, the yellow hard jelly like centre. In boils the yellow centre remains liquid and normally comes out first on bursting. In carbuncles the yellow centre remains until you physically extract it.
Treatment
The only effective treatment is no longer available in Britain. I have had a prescription for 8 years that I have been unable to have made up despite trying many pharmacists, medical supply companies and even one of the companies that used to manufacture them. (They did not even have a record of ever having made them, even though I have an old empty bottle of theirs.)
The original treatment was a compound of tin and tin oxide in tablet form.
Each tablet contains the following:-
- Tin Powder – 0.10625grammes
- Stannous Oxide – 0.01875 grammes
-
Day 1 – 16 tablets (4 + 4 + 4 + 4 )
-
Day 2 – 14 Tablets (4 + 4 + 3 + 3 )
-
Day 3 – 12 Tablets. (3 + 3 + 3 + 3 )
-
Day 4 – 10 Tablets. (3+ 3 +2 + 2 )
-
Day 5 – 8 Tablets. (2 + 2 + 2 + 2 )
-
Day 6 – 6 Tablets. (2 + 2 + 1 + 1 )
-
Days 7 /8/9 and 10 as Day 6
The bracketed numbers indicate the number of tablets to be taken at intervals over the day. It is always best to space them at 6 hour intervals, but it is not crucial.
Why the Cure has been missed by the medical profession.
- Manufactures started marking the the tablets “For use against boils and carbuncles”, but they were totally ineffective against boils. So much for the manufacturers ‘expertise’. Even today they still use the term “for Boils and Carbuncles” on commercial products. Tin and its oxide do not work on boils, antibiotics do not work on carbuncles.
- Doctors were using them for boils, found they did not work, therefore stopped prescribing them. Doctors did not know the differences between boils and carbuncles. It is possible that some doctor had diagnosed a carbuncle as a boil (because it only had a single head) and prescribed stannous oxide, found that it worked, and advised other doctors of this. Later it became obvious that it did not work on real boils and was discontinued.
Having spent many hours over the years discussing carbuncles with members of the medical profession, including dermatologists, I have still not met one who knew the difference. Nor have I met one who had ever had a carbuncle. - Doctors, like many people, generally only learn what they are taught, and what little I have found about carbuncles in medical publications has been very sketchy. Case studies are almost non-existent ( Who wants to read a case study on carbuncles? Therefore why should I do one?) To be honest I’ve not managed to find one yet.
General.
The use of metallic oxides in medicine has received a lot of attention in recent years, particularly in regard to viral infections.
The fact that streptococcus (the claimed cause of boils and carbuncles) is unaffected by tin oxides, clearly indicates that carbuncles are not caused by streptococcus. (This from my experience that anti-streptococcus injections and pills had no effect on carbuncles.) Note that they may have been helpful in that they cleared a lot of streptococcus from the system.
There is a bit of confusion here. When the body is attacked by ‘nasties’, its immune system goes into overdrive. The white blood cells move into action attempting to destroy every kind of ‘nasty’ they can find. The white blood cells will, if possible, kill everything they recognize as a ‘nasty’. Streptococcus is something they recognize and can usually destroy. If you are infected with anything, streptococcus will be found, if only by collateral damage, (they may not be what is causing the problem but will be killed anyway.)
The white blood cells may not even recognize what is actually causing the infection, and therefore ignore it. It is possible that carbuncles are caused by viruses. It may be that streptococcus are carriers of viruses.
It is also possible that the virus responsible for Legionaire’s Disease is the same virus, or similar, to that causing carbuncles. The similarities in origin, attic dust and ventilation dust, would indicate that some further investigation is needed. It would also give the possibility of stannous oxide as a cure for Legionaire’s Disease. Modern ducting systems, using inert materials like plastics or stainless steel, do not have the advantage of having a inner coating of metal oxides (Zinc Oxide) that the traditional galvanised steel has.
It would be nice if Stannous Oxide was available again. because I’ve always had the feeling that carbuncles would eventually kill me.
The only side effect I ever had was that I had to do household tasks sooner.
—————————
Medical Importance of Tin.
TIN by trapper/kcmo .....
Date: 4/29/2011
Hits: 2042
URL:
Tin – Health Effects
Acu-Cell Analysis Acu-Cell Nutrition Acu-Cell Disorders Tin – Health Effects Mineral Ratios
The Clinical Research Resource for Cellular Nutrition using Acu-Cell Technology ™Health Benefits & Toxicity of the Element Tin, and its Effect on Adrenals, Depression and Fatigue
While Tin (Sn) has been established to be an essential trace element for some animals (they won’t grow well without it), some researchers are still unsure of whether tin is essential to human health. Daily dietary intake of tin from various food sources is in the 1 – 3 mg range, which is less than 1/10th of the daily intake obtained years ago before lacquering tin cans, switching to aluminum cans, or, in the more distant past, when tin cups or tin pans were still in use. Since bronze contains copper and tin, the use of tin has been established well past the Bronze Age, several thousand years ago.Rat studies have shown that tin-deficient diets resulted in poor growth, reduced feeding efficiency, hearing loss, and bilateral (male pattern) hair loss. Tipton and Shafer examined tin in human tissue after accidental deaths.
They noted that tin was found in the aorta, brain, heart, kidney, liver, muscle, ovary, spleen, pancreas, testes, stomach, and uterus, but none was found in the thyroid of any victim, while the prostate, which usually shows no other trace element, had tin.
(Is this lack of tin the cause of erectile dis-function and prostate cancer? Brian.
Average concentrations were the same range as cobalt, iodine, chromium, and selenium, which are known vital nutrients. Inorganic tin is capable of entering into biological activity at saline pH, and it is far less toxic than other known vital trace elements such as copper and cobalt. In addition, tin levels do not vary statistically with age, gender, or geographical areas. Misk found traces of tin in the fetal heart and spleen, and higher levels in the liver, while Schroeder and others reported no tin in stillborns.
As mentioned on the Acu-Cell “Tin & Iodine” page – where additional information about tin is found – Tin is associated with iodine in the same way as calcium is associated with magnesium. Tin supports the adrenals, and iodine supports the thyroid, with both subsequently affecting cardiac output: Tin + adrenals control the left side, and iodine + thyroid control the right side. In addition to low Vitamin C and/or Vitamin B1, low tin is a common nutritional cause of low adrenals, which can lead to left-sided cardiac insufficiency. While fatigue or depression may be experienced with cardiac insufficiency of either side, breathing difficulties or asthma are more common with left-sided cardiac insufficiency, and swelling of hands and is more common with right sided cardiac insufficiency, regardless of the cause.
Comparing thousands of patient records since the mid 70’s showed that better than 90% exhibited below normal levels of tin when referenced to the status of all other essential trace minerals, making it the most deficient element compared to any other trace mineral measured. Symptoms associated with low levels of tin typically include depression and/or fatigue, and others.
I had 285 individuals taking part in evaluating tin, some on a short-term basis (about 3 weeks), and others on a long-term basis (1 – 2+ years), resulting in some valuable feedback on various responses encountered, including side effects, although the poor absorption of stannous oxide was a limiting factor in being able to achieve optimal increases of cellular tin in all subjects.
Of those who experienced changes after supplementing tin, negative reactions, e.g. stomach / digestive upsets, or skin reactions were at par, or less compared to the best tolerated trace minerals such as calcium, chromium, or magnesium.
Positive health effects were numerous and included improvements with fatigue, and some forms of depression, with a general increase in energy, well-being and mood. There were also benefits with certain types of headaches, insomnia, asthma, or improvements with digestion, skin, or various aches and pains.
Tin toxicity documented over the last 200 years in humans has been associated with the consumption of foods or beverages that were stored in tinned, un-lacquered containers under long-term, low-pH conditions, and where levels of several hundred to several thousand mg / kg were ingested. Symptoms were limited to mostly gastrointestinal complaints such as nausea, abdominal pain and vomiting, with excess tin being rapidly excreted, and no long-term negative health or toxic effects reported.
There are many causes of depression, some resulting from abnormal brain chemistry, while others are associated with low blood pressure, low thyroid, or low (or high) levels of various essential nutrients such as lithium, calcium, magnesium, copper, sodium, protein, Vitamin B1, Vitamin B6, Vitamin B12, manganese (low blood sugar), among others. Many of these nutrients are well documented in affecting mood, but I have not previously come across any reference to tin until starting to do research on it, and after it helped some patients with depression where any other drug, nutrient, or intervention had failed.Tin is not a panacea for depression — it will not work when other chemical imbalances are involved, but it can be the missing link when most other attempts to resolve depression have failed; essentially involving low, or malfunctioning adrenals. For the same reason, some cases of asthma – particularly when related to low adrenals and subsequent left-sided cardiac insufficiency – respond to tin as well.
Tin (as stannous fluoride) is found in some toothpastes, and it has been used in the form of stannous chloride as a chemical preservative. It is also added to asparagus to improve its taste, while in some countries it has been utilized as a remedy for intestinal parasites.
Some herbal sources of tin (in the highest to lowest order) are doggrass, juniper, bilberry, milk thistle, dulse, lady slipper, althea, valerian, Irish moss, nettle, barberry, yarrow, blessed thistle, red clover, yellow dock, kelp, licorice, devils claw, pennyroyal, and senna. ¤General recommendations for nutritional supplementation: To avoid stomach problems and promote better tolerance, supplements should always be taken earlier, or in the middle of a larger meal. When taken on an empty stomach or after a meal, there is a greater risk of some tablets causing irritation, or eventually erosion of the esophageal sphincter, resulting in Gastroesophageal Reflux Disease (GERD). It is also advisable not to lie down immediately after taking any pills. When taking a very large daily amount of a single nutrient, it is better to split it up into smaller doses to not interfere with the absorption of other nutrients in food, or nutrients supplemented at lower amounts.
___________________
Copyright © 2011 Acu-Cell – Element Tin: Health Benefits & ToxicityDietary Reference Intake (DRI) is the latest term replacing daily dietary reference values such as:
Adequate Intake (AI *), Nutrient Reference Value (NRV), Tolerable Upper Intake Level (UL), Estimated
Average Requirements (EAR), and Recommended Dietary Allowance / Intake (RDA / RDI).Tin – (Stannous Oxide):
DRI (RDA): none
18 years + (suggested minimum) 10-20mg
Therapeutic Range: 25mg – 250mg
Estimated daily intake of tin from food and water (excluding canned food) is 1mg – 3mg per day.
Cellular / Intracellular Attributes, Functions and Interactions:
Tin Synergists:
Nickel, iodine, Vitamin B1, Vitamin C,Tin Antagonists:
Iron, calcium, copper, chloride,
Vitamin B2, Vitamin E, [bismuth, zinc].Low Levels / Deficiency – Symptoms and/or Risk Factors:
Fatigue, depression, low cardiac output (left side), low adrenals, shortness of breath, asthma, headaches, insomnia.
In Animals: Low tin results in poor growth, alopecia / bilateral hair loss, hearing loss, and reduced feeding efficiency.
High levels / Overdose / Toxicity / Negative Side Effects – Symptoms and/or Risk Factors:
Skin rash, stomach complaints, nausea, vomiting, diarrhea, abdominal pain, headache, palpitations.
Tin Sources:
Tinned / canned foods, cereal grains, dairy, meat, vegetables, seaweed, licorice, some toothpastes. ¤——————————————–
Extract from BBC news item. 1 October 2011
Copper fixtures could help hospitals combat infections such as MRSA, scientists say, because of its anti-bacterial and anti-viral properties.
In Trafford General Hospital, copper door handles and work surfaces are replacing stainless steel in the fight against the superbug.
Combined with meticulous hygiene, the new fittings have contributed to the hospital’s MRSA-free status for the past two years.
Copper oxide, zinc oxide, stannous oxide. For over 100 years Metal oxides have been known for their medical properties. When I was a child we knew that it was safe to suck copper coins. Zinc oxides were used in dressings and ointments and tin oxide was used for carbuncles. Why has the medical profession been so slow?
SEE ALSO;
Tin, BPA, BPS and Phthalates. Brian Williams
Author